Introduction
Dental implants have become the best alternative for replacing missing teeth (Moraschini et al., 2015). However, long-term implant success depends not only on proper treatment planning and execution, but also on continuous monitoring and maintenance over time (Berglundh et al., 2017).
Following the placement of a dental implant, two major biological events occur during the healing process. The first is osseointegration, which refers to the direct structural and functional connection between newly formed bone and the implant surface. The second phenomenon is the formation and maturation of peri-implant soft tissues around a transmucosal abutment, establishing a protective interface between the intraosseous implant and the oral cavity. This process typically occurs between 8 and 12 weeks after the placement of the transmucosal abutment (Rios-Osorio et al., 2024).
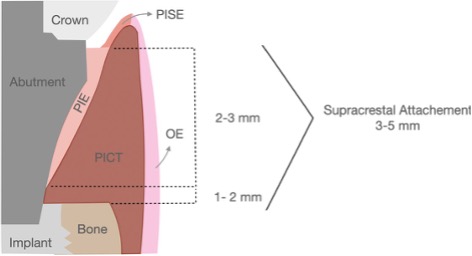
The peri-implant mucosa is characterized by three types of stratified squamous epithelium: the peri-implant epithelium (PIE), the peri-implant sulcular epithelium (PISE), the oral epithelium (OE) and the peri-implant connective tissue (PICT) (Alsusa I et al., 2016) (Figure 1). Together they form a biological seal. The PICT plays a crucial role in protecting the implant interface from various noxious agents, such as plaque formation and chemical irritants. It also facilitates the supply of nutrients through its vascular network, contributes to stabilizing the apical migration of the peri-implant epithelium and helps prevent bone resorption. (Alsusa I et al., 2016; Zheng et al., 2021)

Although implants behave similarly to natural teeth, their surrounding tissues are biologically different. One of the main differences in anatomical features is the absence of the periodontal ligament at the bone-to-implant interface. The other important structural difference is found in the connective tissue arrangement of the peri-implant mucosa where collagen fibers run parallel to the long axis of the implant abutment surface rather than inserting into it. (Berglundth et al., 2018; Araujo et al., 2024). In addition, the peri-implant connective tissue (PICT) has a reduced vascular supply compared with periodontal connective tissue, resulting in lower vascularization and reduced nutritional support (Renvert et al., 2018; Monje et al., 2022). The absence of a true connective tissue attachment to the implant surface may facilitate bacterial penetration into the peri-implant mucosa and the underlying alveolar bone, increasing the susceptibility of peri-implant tissues to peri-implant diseases (Pokrowiecki et al., 2017).
The European Federation of Periodontology (EFP) and the American Academy of Periodontology (AAP) have introduced a classification for peri-implant diseases and conditions. According to this classification, peri-implant health is defined as a state in which immune surveillance maintains homeostasis and the clinical stability of the peri-implant mucosa. Clinically, peri-implant health is characterized by the absence of erythema, bleeding on probing (BOP), inflammation, and suppuration in the tissues surrounding a dental implant (Berglundh et al., 2018).
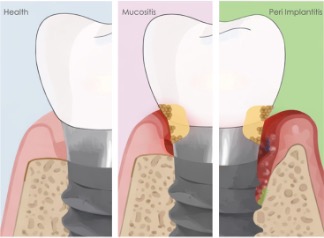
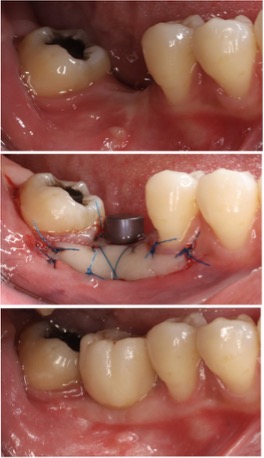
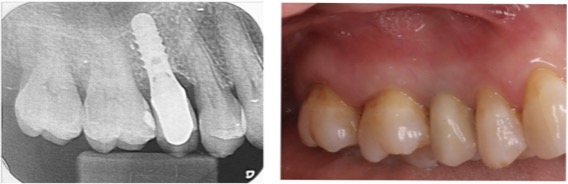
The two main biological conditions affecting peri-implant tissues are peri-implant mucositis and peri-implantitis, both induced by biofilm accumulation. Peri-implant mucositis presents as inflammation of the peri-implant mucosa without bone loss and is considered a reversible condition when diagnosed and treated early. If the local and systemic etiological factors responsible for inflammation are not controlled, peri-implant mucositis may progress to peri-implantitis. Peri-implantitis is characterized by inflammation associated with progressive loss of supporting bone after functional loading and may ultimately lead to implant failure if left untreated (Berglundh et al., 2018; Schwarz et al., 2017) (Figure 2).
The aim of this article is to provide a simple and practical checklist for dentists to apply at every recall visit. By following a structured approach, clinicians can facilitate the early diagnosis of peri-implant diseases, improve patient compliance with supportive care, and reduce the risk of late biological and mechanical complications. Early detection and timely intervention are essential to prevent disease progression, preserve implant longevity, and ultimately ensure patient satisfaction and quality of life.
For long-term implant success, one of the most important habits we can develop is consistent clinical monitoring:
1. Probing depth and bleeding on probing:
These measurements are performed using a periodontal probe with light force (approximately 0.15 N) and provide valuable information about the condition of the peri-implant tissues (Cha et al., 2019). The probe should be inserted parallel to the long axis of the implant and walked circumferentially around it, in a manner similar to probing around natural teeth. When performed correctly, gentle probing is considered safe and does not damage the peri-implant seal. Ideally, measurements should be recorded at every recall visit and compared with baseline values obtained at the time of prosthesis delivery (Abrahamsson et al., 2006).
However, probing around over-contoured suprastructures (crowns or implant prostheses) presents significant clinical challenges, as it may hinder proper probe angulation and lead to inaccurate readings, false-positive diagnoses, or increased tissue trauma. In such cases, removal of the prosthesis may be necessary to obtain accurate measurements and allow proper debridement of the implant surface (Monje et al., 2024).
In healthy peri-implant tissues, no bleeding or suppuration is expected during gentle probing, and probing depths should remain stable over time. Bleeding on probing (BOP) is one of the earliest clinical signs of inflammation and is strongly associated with peri-implant mucositis, while probing depth (PD) helps assess the stability of the peri-implant soft tissues and may indicate changes in the supporting bone (Schwarz et al., 2017).
Peri-implant mucositis is characterized by inflammation of the peri-implant mucosa with bleeding and/or suppuration on probing but without progressive bone loss. In contrast, peri-implantitis presents with similar inflammatory signs accompanied by increased probing depths and radiographic bone loss. In advanced cases, the implant surface could be exposed, and implant threads may be detected during probing due to vertical bone loss. The onset of peri-implantitis may occur early, sometimes within the first three years of function, and disease progression may be rapid (Rios-Osorio et al., 2024).
Therefore, probing findings should always be interpreted in conjunction with a careful visual examination of the peri-implant tissues, including the assessment of the soft tissue color, consistency, integrity, and the presence of suppuration and/or crevicular fluid.
2. Oral hygiene of the patient
Long-term implant success is closely linked to effective plaque control. As explained before, peri-implant tissues are particularly vulnerable to biofilm accumulation and, as a result, inflammatory changes may develop more rapidly around implants than around natural teeth. Patient self-performed plaque control therefore represents one of the most important factors in the prevention and management of peri-implant diseases (Herrera et al., 2023; Perussolo et al., 2024).
Clinicians should carefully assess the patient’s oral hygiene around implants. This evaluation should include inspection of the peri-implant mucosa, assessment of plaque accumulation, and identification of areas that may be difficult for the patient to clean (Perussolo et al., 2024). Patient education is essential and instructions should be tailored to the type of restoration, whether it is a single implant crown, implant-supported bridge, or full-arch prosthesis.
Several devices can be used to improve plaque control around implants, including manual or powered toothbrushes, single-tuft brushes, interdental brushes, dental floss, oral irrigators, and antimicrobial mouthrinses. Interdental brushes of an appropriate size
are often more effective than floss for cleaning around implants because they can better access the peri-implant embrasures (Chongcharoen N et al., 2012).
When floss is used, it should be applied carefully, particularly in cases with exposed implant threads or prosthetic misfit, to avoid leaving floss fibers on the implant surface, which may contribute to plaque accumulation and inflammation. Newer interproximal cleaning devices have also been developed, such as waist-shaped interdental brushes, which have shown improved plaque removal compared with conventional straight brushes (Van Velzen et al., 2016).
Oral irrigators, also known as dental water jets or water flossers, deliver pulsating fluid under controlled pressure and may be especially useful in situations where access for oral hygiene is limited, such as around complex implant restorations (Tütüncüoğlu et al., 2022).
Professional maintenance is equally important in the prevention and management of peri-implant disease. Regular professional removal of biofilm and calculus, reinforcement of oral hygiene instructions, and monitoring of tissue response are essential components of long-term implant care (Jepsen et al.,2015).
When plaque control is effective, peri-implant mucositis is reversible. However, if biofilm accumulation persists, disease progression and the development of peri-implantitis become more likely (Figure 3).

3. Soft tissue assessment around implants
Healthy peri-implant mucosa should resemble healthy gingiva in color, consistency, and absence of inflammation (Parpaiola et al., 2015). However, beyond visual inspection, several soft tissue parameters should be evaluated before implant placement and during maintenance visits, as they may influence long-term implant stability (Figure 4).
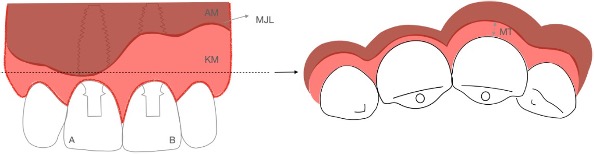
Peri-implant keratinized mucosa width (KMW) refers to the vertical dimension of keratinized soft tissue extending in an apico-coronal direction from the mucosal margin to the mucogingival junction. A KMW of ≥2 mm is generally considered adequate. When sufficient keratinized mucosa is present and part of it is attached to the underlying alveolar bone, the peri-implant soft tissue collar is more firmly adapted to the transmucosal prosthetic components. This results in a more stable mucosal seal that may help prevent the apical migration of bacteria. In contrast, when the width of keratinized mucosa is less than 2 mm, the tissue tends to be more fragile and less stable, which may increase the risk of inflammation and progressive apical migration of the mucosal margin (Monje et al., 2022). Additionally, vestibular depth should be evaluated. A shallow vestibule (<4 mm) may compromise hygiene access and soft tissue stability (Monje et al., 2022) (Figure 5).
Mucosal thickness (MT) is the horizontal dimension of the peri-implant soft tissue, which may or may not be keratinized. The relevance of MT is particularly critical in the most coronal region of the peri-implant mucosa. Current evidence suggests that a minimum of 2 mm is often associated with favorable outcomes (Suarez-Lopez Del Amo et al. 2016). Thicker MT is associated with peri-implant marginal bone stability (Thoma et al,. 2018) (Figure 6).

The peri-implant supracrestal tissue height (STH) is the vertical dimension of the peri-implant soft tissue extending from the mucosal margin to the crestal bone surrounding a dental implant (Monje et al., 2022). It includes the peri-implant sulcular epithelium, the junctional epithelium, and the supracrestal connective tissue. The dimensions of this soft tissue complex depend on factors such as implant design and the anatomical location of the implant. A supracrestal tissue height of less than 3 mm is generally considered deficient (Linkevičius et al., 2009; 2010; 2018). In sites with limited baseline STH, the establishment of this biological dimension may occur at the expense of physiologic crestal bone remodeling (Suárez-López Del Amo et al., 2016) (Figure 7).
Around implants, inflammation tends to progress in a more vertical and faster pattern once established. For this reason, early detection of soft tissue changes is critical for long-term success.
When should the patient be referred to a periodontist?
- When the width of keratinized mucosa is less than 2 mm and signs of inflammation are present.
- When the vestibular depth is shallow and the patient experiences discomfort during oral hygiene.
- When the peri-implant mucosal thickness is less than 2 mm and the patient reports difficulty or discomfort maintaining adequate peri-implant hygiene.
- When the supracrestal tissue height (STH) is less than 3 mm and signs of inflammation or progressive crestal bone remodeling are present.
4. Prosthetic integrity
The design and contours of implant-supported prostheses may create areas that are difficult to clean, allowing biofilm to accumulate and potentially initiate peri-implant disease (Serino C Ström, 2009). In addition, iatrogenic factors such as poor marginal fit and submucosal excess cement can provide niches for biofilm retention. Prostheses with compromised fit but supra mucosal margins that remain accessible for cleaning may represent a moderate risk for peri-implant disease (Kordbacheh Changi et al., 2019).
Mechanical complications may also precede biological ones. For example, a loose abutment screw can create a micro gap at the implant–abutment interface, favoring bacterial colonization and inflammation. Similarly, over-contoured restorations, deep emergence profiles, or poorly positioned crown margins may compromise plaque control and increase the risk of peri-implant mucositis (Chankhore et al., 2023).
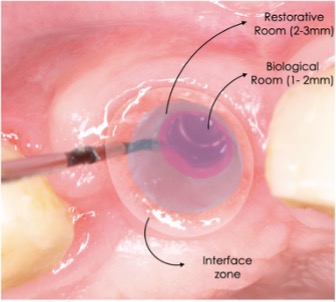
Restorative design also plays an important role in maintaining peri-implant tissue health. The most apical portion of the restoration, often referred to as the biological room, corresponds to the area where muco integration occurs and where the soft tissue seal forms to protect the underlying bone. Materials commonly used in this zone include titanium or zirconia due to their favorable biocompatibility. Coronal to this area lies the restorative room, which extends from the biological room to the free gingival margin. This region may be restored using materials such as glass ceramics, zirconia, lithium disilicate, composites, polymers, or PMMA. Its main purpose is to create a harmonious transition between the restoration and the surrounding soft tissues while maintaining adequate access for hygiene. Proper morphology, appropriate material selection, and prosthetic design are essential to support soft tissue stability, esthetics, and long-term maintenance of implants (Fabris et al., 2025) (Figure 8).
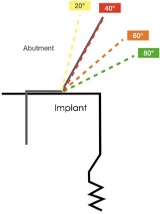
Emergence profile also influences peri-implant tissue health. Wider restorative emergence angles of greater than 40° have been associated with increased peri-implant inflammatory cell infiltration, particularly at buccal sites, potentially compromising long-term tissue stability (Strauss et al., 2026) (Figure 9).
In the context of the IDRA system, the term cleanable refers to the accessibility of the prosthesis for both the clinician and the patient. The patient’s ability to maintain adequate hygiene depends on individual skills and manual dexterity, which may change over time (Heitz-Mayfield et al.,2019).
What to check
- Screw stability (tighten if necessary, according to the manufacturer’s guidelines)
- Presence of ceramic chipping, framework fractures or wear (Figure 10)
- Restorative margins for excess cement
- Emergence profile and accessibility for oral hygiene
- Material of the abutment and crown

5. Occlusal factors
Mechanical stress generated during biting and chewing plays an important role in the long-term stability of implant-supported restorations. The way occlusal forces are distributed through the prosthesis, implant, and surrounding bone may influence peri-implant tissue health (Chankhore et al., 2023).
Factors such as crown morphology, implant angulation, prosthetic materials, and the choice between cement or screw-retained restorations can influence how forces are transmitted to the supporting structures. Poorly distributed contacts, heavy centric contacts, cantilevers, or parafunctional habits such as bruxism may increase the risk of screw loosening, ceramic fractures, and prosthetic component fatigue over time (Delgado-Ruiz et al., 2019).
Occlusion should also be routinely evaluated during implant maintenance visits. Unlike natural teeth, implants lack a periodontal ligament and therefore have reduced proprioceptive feedback compared with natural teeth. When forces (especially non-axial loading) are not properly controlled, localized stress concentrations may occur at the implant–bone interface, potentially contributing to bone remodeling, and mechanical complications over time may influence marginal bone stability when combined with inflammation (D’Amico et al., 2020).
During recall visits, clinicians should assess occlusal contacts, prosthetic mobility, wear facets, fractures, fremitus, and any signs of parafunction. In patients presenting with bruxism or excessive occlusal forces, the use of a night guard may be indicated. Occlusal adjustments should aim for light, well-distributed contacts in maximum intercuspation and minimal non-axial loading, particularly in posterior regions (Figure 11).
What to check at every appointment:
- Assess occlusal contacts, wear facets, fractures, fremitus, and signs of parafunction (e.g., bruxism), and verify whether the patient uses a night guard.
- Non-axial loading
- Repeated screw loosening or screw fracture
- Prosthetic mobility

6. Radiographic monitoring
Radiographic imaging, together with clinical parameters, is essential for the proper diagnosis of peri-implant disease and plays a key role in long-term implant maintenance.
Radiographs provide important information about the status of peri-implant bone. They allow clinicians to detect early demineralization and visualize initial or progressive marginal bone loss. In many cases, radiographic changes may represent the first indication of disease progression in implants that appear clinically stable (Sahrmann et al., 2024).
Ideally, once the implant has been restored, a baseline intra-oral radiograph (periapical or bitewing) should be obtained to document the mesial and distal marginal bone levels. Together with probing measurements, baseline records are critical for detecting early changes in peri-implant tissues.
Radiographic signs of peri implant health (Figure 12):
- Stable marginal bone levels over time. Marginal bone levels are typically established at or slightly apical to the most coronal portion of the endosseous part of the implant.
- No progressive bone loss beyond initial remodeling. This initial remodeling usually takes place during the first 3–12 months after implant placement or loading and should not be interpreted as pathological bone loss. Instead, it represents a normal biological response to surgical trauma, implant design, and the establishment of the peri-implant soft tissue seal.
Radiographic signs of peri-implantitis:
- When clinical signs such as bleeding on probing are present but radiographs show stable bone levels, the condition is consistent with peri-implant mucositis (Berglundh et al., 2017). In contrast, radiographic evidence of progressive marginal bone loss, together with increased probing depths or mucosal recession compared with baseline, and bleeding on probing and/or suppuration, is indicative of peri-implantitis (Berglundh et al., 2017).
In the absence of baseline data, peri-implantitis may be diagnosed when the following findings are present:
- Bleeding on probing
- Probing depths ≥6 mm
- Marginal bone levels ≥3 mm apical to the most coronal portion of the endosseous implant
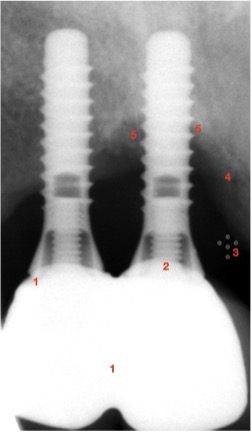
- Peri-implant bone loss is often circumferential and may occur early, sometimes within the first three years of function; clinical and intraoperative studies further show that peri-implantitis defects are most commonly characterized by a combined supra- and intrabony configuration, with a predominance of uniform bone resorption affecting all aspects of the implant, while less frequent patterns include buccal dehiscence-type defects, supporting the concept that these lesions typically progress circumferentially rather than as isolated defects (Schwartz et al 2018, Berglundh et al., 2017) (Figure 13).
Intraoral radiographs are considered the first choice for assessing peri-implant sites because they provide sufficient spatial resolution, relatively low radiation exposure, and high sensitivity for detecting peri-implant bone defects (Kuhl et al., 2016).
Also, they provide additional information about the prosthetic components and surrounding bone structures. Radiographs can reveal additional findings such as loss of interproximal contacts, ceramic chipping, or fractures of the prosthetic framework.
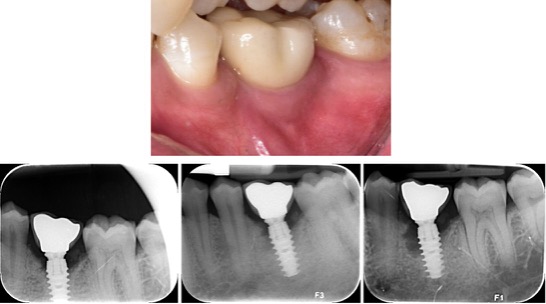
What to check in a periapical image at an appointment? (Figure 14)
- Cement remnants, chipping or misfit of the prosthetic crown.
- Transmucosal components: The implant abutment interface and the fit of the prosthetic restoration. An improper fit between prosthetic components may indicate mechanical complications.
- Loose particles of grafted autologous bone or synthetic bone substitutes may be visible in the peri-implant mucosa and appear radiographically as small radiopaque structures overlying the crestal bone. Recognizing them helps avoid misdiagnosis and supports accurate peri-implant assessment.
- Marginal bone morphology and density: A thin, continuous cortical bone line clearly delineated from the underlying bone suggests a stable bone structure. This appearance generally indicates a stable peri-implant condition.
- Bone-to-implant interface: An increase in bone density at the interface after functional loading may represent a physiologic adaptation to occlusal forces (Sahrmann et al., 2014). Such densification is usually observed during the first year after loading and is associated with absolute or relatively high loading forces.
While highly mineralized (cortical) bone provides good mechanical stability, it is less vascularized and biologically active, reducing its ability to maintain tissue homeostasis or adapt to increased occlusal or parafunctional loading, thereby increasing the risk of connective tissue encapsulation around the implant. This process may be reflected in radiographic changes that begin at the implant shoulder and progress apically without initial clinical symptoms.
When are panoramic radiographs useful?
This option should only be considered when intra-oral radiographs are not feasible, such as when the area of interest exceeds the mesio-distal dimensions of an intra-oral image or when additional vertical information is required, for example, in cases involving zygomatic implants, sinus floor augmentation where a periapical radiograph is insufficient, or multiple implants in both jaws. Panoramic radiographs may also be useful in patients with limited mouth opening, flat palates, or a shallow floor of the mouth (Kuhl et al., 2016).
Conclusion
Implant success in the long term is rarely a matter of chance. Most biological and mechanical complications develop gradually, and early signs can often be detected during routine maintenance visits. A structured clinical approach at every recall: assessing probing depth, bleeding on probing, oral hygiene, soft tissue conditions, prosthetic integrity, occlusion, and radiographic bone levels allows clinicians to identify problems early on. Around implants, inflammation should never be considered normal and should always prompt further evaluation.
The key is not only to detect disease but to intervene at the appropriate time. Peri-implant mucositis is reversible when managed early, while peri-implantitis is more complex and less predictable once bone loss occurs. Therefore, the use of a simple and consistent checklist during maintenance visits supports early diagnosis, improves patient compliance, and contributes to the long-term stability of implant therapy.