
Introduction
Dental implant therapy is a widely accepted treatment modality for the replacement of missing teeth, demonstrating long-term survival rates of approximately 95% over 10 years (Roccuzzo et al., 2010; Fischer et al., 2012; Buser, 2012). When implant survival is considered the primary outcome, implant therapy can be regarded as highly reliable (Fischer, 2012; Mertens, 2012; Degidi, 2012).
Despite these favorable outcomes, biological and technical complications remain frequently associated with inadequate integration of surgical and restorative planning (Salvi et al., 2004; Serino et al., 2009; Sanz- Martín et al., 2020). Although implant dentistry is traditionally described as a restorative-driven discipline, clinical practice often reveals a fragmented approach in which surgical and restorative phases are conducted sequentially rather than collaboratively. Implant positioning dictated primarily by available bone, or restorative planning constrained by prior surgical decisions, may compromise esthetics, function, maintenance, and long-term stability.
Contemporary implant dentistry increasingly emphasizes interdisciplinary, patient-centered treatment planning, recognizing that surgical and restorative decisions are interdependent and collectively influence predictability, treatment outcomes, and overall treatment success. Understanding this bidirectional relationship is therefore essential for achieving sustainable and satisfactory implant rehabilitation.
Given the narrative and practice-oriented nature of this article, a structured systematic search strategy was not applied. Instead, the literature was consulted iteratively according to the clinical topics addressed throughout the manuscript. All references were selected from peer-reviewed journals indexed in major scientific databases, primarily PubMed, prioritizing high-quality, relevant, and contemporary evidence to support each discussed concept. This approach aimed to ensure that the cited literature reflects current best evidence while maintaining clinical applicability to daily implant practice.
How surgical decisions impact restorative outcomes
This section addresses how seemingly minor surgical decisions can have significant long-term implications for prosthetic treatment.
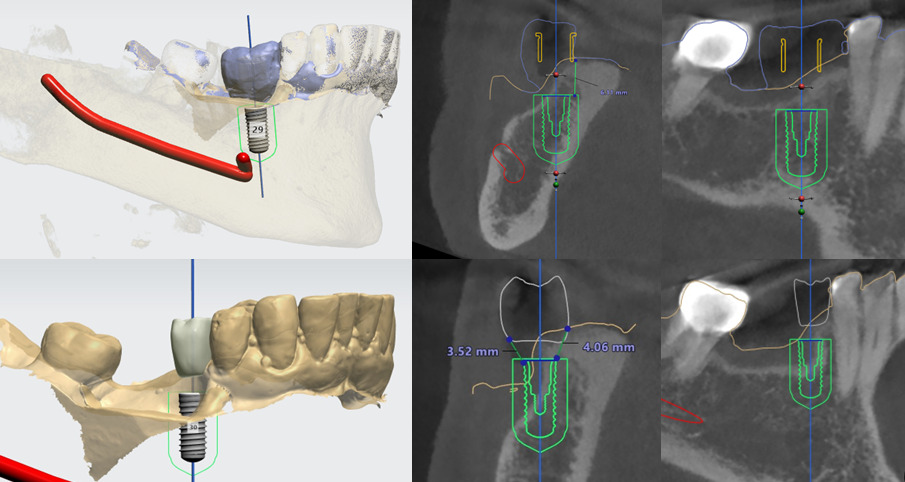
Implant depth and angulation
Once the surgical position is determined, even minimal deviations in implant depth or angulation may significantly affect prosthetic fabrication, hygiene access, and long-term esthetic stability (Figure 1). On the contrary, placing the implant too deep might require a narrow connection, which might compromise the mechanical integrity of the restoration against occlusal loads (Buser et al., 2004; Buser et al., 2017).
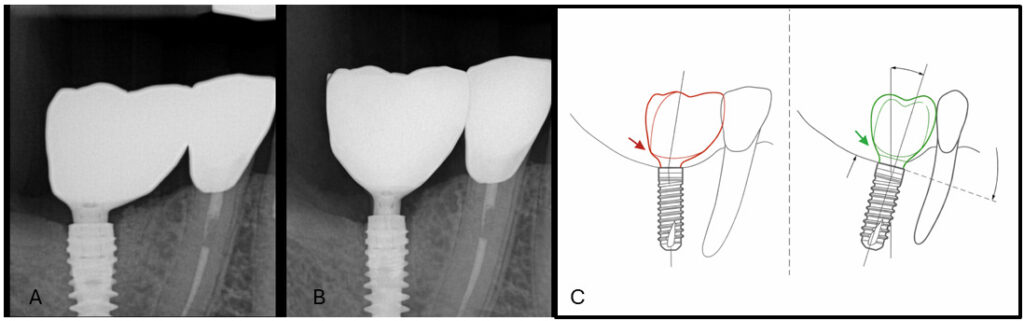
Implants placed too deeply may not present immediate esthetic complications but can predispose to peri-implant mucosal inflammation due to limited hygiene access (Serino et al., 2009). Conversely, excessively superficial placement, particularly in one-piece implants, may result in visible implant shoulders and significant esthetic compromise, sometimes requiring implant removal or modification (Blanes et al., 2007).
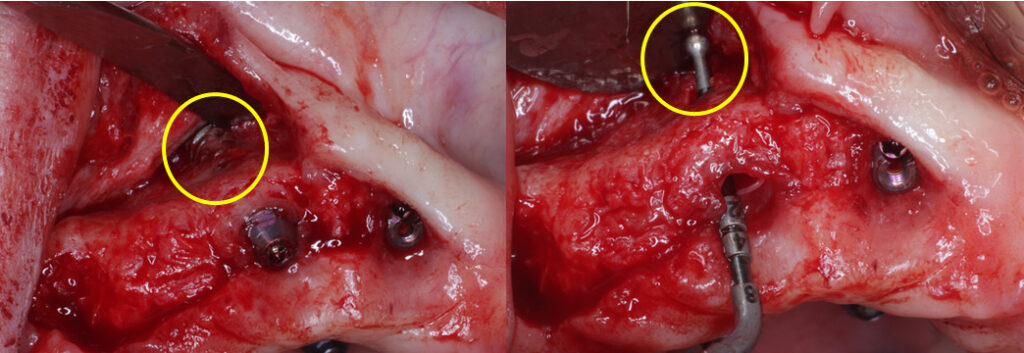
Angulation errors may lead to over-contoured prostheses that hinder effective cleaning. Peri-implantitis has been associated with limited hygiene access, whereas adequate accessibility is rarely linked to disease (Yi et al., 2020; Serino et al., 2009). Additionally, poor adherence to maintenance programs is associated with higher implant failure rates (Roccuzzo et al., 2010) (Figure 2).

In the orofacial dimension, excessively facial implant positioning is strongly associated with gingival recession (Evans et al., 2008), while excessive palatal placement often necessitates prosthetic over contouring, thereby increasing the risk of inflammation.
Clinical implications: Millimeters in surgical positioning translate into long-term daily challenges in prosthetic maintenance.
Hard and soft tissue requirements
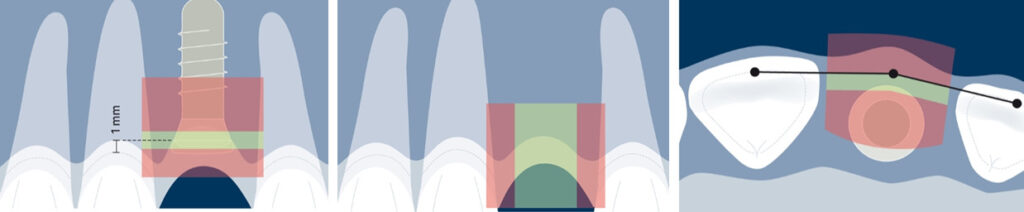
Inadequate management of hard and soft tissues during surgery may compromise papilla preservation, emergence profile development, and overall esthetic integration, ultimately increasing prosthetic complexity (Pelekos et al., 2023; Ramanauskaite et al., 2022; Sun et al., 2024). When residual bone does not permit implant placement in accordance with restorative demands, prosthetically guided bone augmentation should be performed either before or simultaneously with implant placement to re-establish optimal bone architecture (Monje et al., 2023). In addition, atraumatic surgical preparation is essential for predictable osseointegration, requiring careful heat control (Orgev et al., 2021) and sequential drilling protocols to minimize bone injury (Eriksson & Albrektsson et al., 1983).
Soft tissue conditions also directly influence restorative outcomes. Recent long-term evidence has shifted the focus from implant survival alone to peri-implant health and tissue stability. A 20-year prospective study demonstrated significantly greater marginal bone loss, bleeding on probing, mucosal recession, and peri-implantitis in implants lacking keratinized mucosa. Peri-implantitis occurred in 25% of implants without keratinized tissue compared with 4.2% in sites with adequate or grafted mucosa (Roccuzzo et al., 2025). These findings, supported by recent clinical evidence (Stefanini et al., 2023; Mancini et al., 2023), highlight the protective role of adequate peri-implant soft tissue and reinforce the importance of soft tissue augmentation when necessary to support long-term peri-implant health and restorative stability (Sun et al., 2024).
Overall, careful management of hard and soft tissue during the surgical phase is fundamental to facilitating restorative design, maintaining peri-implant health, and ensuring long-term stability (Sun et al., 2024) (Figure 3).
Clinical implications: Restorative outcomes rely heavily on the quantity and quality of tissues preserved during surgery.
How restorative planning impacts surgical implant position
This section highlights how restorative decisions made during the planning phase can significantly affect surgical complexity and outcomes.
Restorative-driven position versus available bone
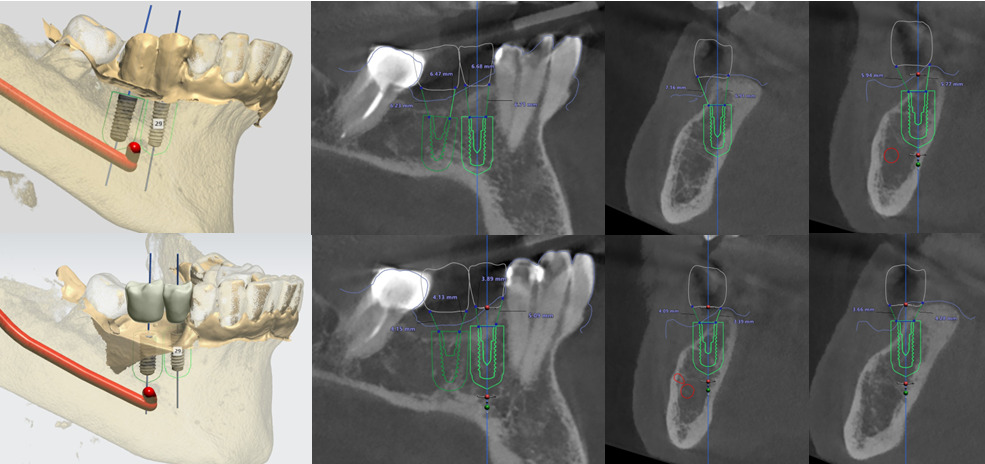
For optimal outcomes, implant placement should be guided by prosthetic objectives rather than bone availability alone. The ideal three-dimensional implant position is dictated by the planned restoration, including the emergence profile, occlusal scheme, esthetic requirements, and long-term maintenance considerations (Pelekos et al., 2023) (Figure 4).
Nonetheless, in clinical practice, severely atrophic sites often lead to implant placement based primarily on residual bone volume, sometimes without prosthetically guided bone augmentation. Consequently, implants may be malpositioned relative to the ideal restorative position, leading to a range of peri-implant hard and soft tissue deficiencies, both vertically and horizontally (Berglundh et al., 2018).
Such conditions are associated with reduced patient satisfaction, as prosthetic restorations supported by poorly positioned implants often result in compromised functional and esthetic outcomes and limit the patient’s ability to perform effective plaque control (Zucchelli et al., 2020; Sanz Martín et al., 2020; Tavelli et al., 2022). Inadequate prosthetic planning may lead to unfavorable implant angulation, suboptimal emergence profiles, and the need for angled abutments or compensatory prosthetic designs (Figure 5).
Implants placed too close to adjacent teeth may jeopardize interproximal bone height and papilla support, thereby affecting esthetic symmetry (Tarnow et al., 2003; Lee et al., 2005). Similarly, deviations in the orofacial dimension can result in overcontoured restorations or soft tissue instability. Deviations from ideal three-dimensional implant positioning are among the primary contributors to esthetic complications (Morton & Beagle, 2019; ITI Academy module on Etiology of Esthetic Complications).
Clinical implications: The prosthesis should define implant positioning, not the available bone alone.
The impact of restorative design on implant number and distribution
The restorative design – whether a single crown, fixed partial denture, or full-arch rehabilitation – directly determines implant number, diameter, and spatial distribution. Implant selection should not be based solely on available bone, but primarily on restorative design, prosthetic morphology, and functional load requirements. In this context, restorative planning dictates surgical positioning (Figure 6).
For single crowns, one implant per missing tooth is generally indicated to reproduce natural anatomy and ensure the appropriate emergence profile and occlusion. Although survival rates are high (Jung et al., 2012), prosthetic complications remain common (Rinke et al., 2015), often related to force distribution and platform dimensions (Gealh et al., 2011). While implant diameter does not significantly influence survival in posterior regions (Blanes et al., 2007), discrepancies between crown width and implant platform may increase non-axial loading, particularly in unfavorable crown-to-implant ratios (Thoma et al., 2021).
In fixed partial dentures, the number and distribution of implants depend on span length and the presence of a cantilever. Although cantilevers are not consistently associated with marginal bone loss (Wennstrom et al., 2004; Halg et al., 2008), they are linked to higher rates of mechanical and prosthetic complications, reinforcing the need for prosthetically guided load distribution. Full-arch rehabilitations require even more strategic implant positioning to control distal cantilevers and optimize anterior–posterior spread (Storelli et al., 2018), as complication patterns differ from those observed in shorter-span prostheses (Londhe et al., 2020).
Across all restorative designs, implant number and distribution must anticipate occlusal force magnitude and concentration to ensure biomechanical stability and long-term predictability.
Clinical implications: Prosthetic design determines surgical strategy, implant distribution, and biomechanical load control. Surgical implant placement must therefore be restoratively guided to ensure predictable restorative outcomes.
How surgical and restorative decisions impact the overall patient rehabilitation
This section emphasizes the importance of viewing implant therapy as an integrated, patient-centered process.
Treatment duration, morbidity, and cost
A lack of integration between surgical and prosthetic planning often may contribute to additional procedures, prolonged treatment times, and increased biological and financial costs (Berglundh et al., 2018). When implant positioning is guided primarily by bone availability rather than restorative requirements, corrective interventions-such as bone grafting, prosthetic redesign, or component customization-may become necessary, thereby extending the rehabilitation timeline. Although immediate placement and loading protocols may reduce treatment duration, inadequate case selection or insufficient primary stability can result in complications that ultimately delay treatment completion.
Fragmented planning also increases biological morbidity. Multiple surgical interventions, improper three-dimensional positioning, or unfavorable load distribution may compromise peri-implant tissue health and elevate the risk of mechanical and biological complications (Zitzmann et al., 2008). These factors not only affect osseointegration and long-term stability but may also require additional corrective procedures.
Financial implications accompany these clinical challenges. Additional surgeries, prosthetic remakes, and increased chair time raise direct costs, while extended treatment duration and complexity impose indirect burdens on patients. Biomechanical consequences-such as unfavorable cantilevers, stress concentration, or reliance on cement-retained restorations due to implant malposition-may further compromise long-term sustainability.
Ultimately, patients perceive implant therapy as a continuous experience rather than as separate surgical and restorative phases. Treatment duration, number of interventions, comfort, cost, and predictability collectively determine satisfaction.
Clinical implications: Patients experience treatment as a unified experience rather than as isolated clinical phases.
Load distribution and biomechanical behavior
Implant positioning and prosthetic design directly influence load direction, stress distribution, and micromovements at the bone–implant interface. Inadequate integration between surgical and restorative planning increases the risk of mechanical complications, such as screw loosening, abutment fracture, or crown failure, as well as marginal bone loss (Roccuzzo et al., 2010; Serino et al., 2009).
The long-term success of implant-supported rehabilitation depends on controlled load transfer (Nissan et al., 2010) (Figure 7). Surgical decisions-including implant angulation, depth, and distribution-must align with restorative planning, encompassing prosthetic design, occlusal scheme, and crown-to-implant ratio. Misalignment between these factors may result in localized overload, peri-implant tissue inflammation, and premature prosthetic failure (Berglundh et al., 2018; Buser et al., 2012). Conversely, coordinated planning optimizes force distribution, reduces biomechanical stress, and enhances prosthetic durability and tissue stability.

Patient-specific factors, such as masticatory patterns, bite force, and parafunctional habits, further emphasize the need for integrated planning. Anticipating functional demands and aligning surgical and restorative strategies help ensure biomechanical predictability, protect peri-implant tissues, and improve overall patient satisfaction.
Clinical implications: Biomechanical predictability depends on coordinated surgical and prosthetic planning.
Selecting the treatment approach and managing patient expectations
Implant therapy is a predictable and well-established modality for tooth replacement; however, as its use has expanded, patient expectations regarding functional and esthetic outcomes have similarly increased (Belser et al., 2004). In this context, selecting the appropriate treatment approach requires careful consideration of both clinical conditions and patient-related factors. Esthetic expectations, particularly in the esthetic zone, significantly influence case complexity, as reflected by the ITI SAC Classification (Figure 8).
High esthetic demands require precise three-dimensional implant positioning and careful management of hard and soft tissues to achieve harmonious integration among the prosthesis, peri-implant tissues, and adjacent dentition. Failure to incorporate restorative requirements into surgical planning may compromise gingival symmetry, papilla support, and prosthetic contours, potentially necessitating additional corrective procedures.
Treatment planning must also consider the timing of implant placement and loading protocols, as these decisions directly influence treatment duration, prosthetic workflow, and patient experience. Implant placement may be performed immediately after extraction (Type 1), early after partial healing (Type 2 or 3), or in a fully healed site (Type 4), depending on factors such as socket morphology, bone quality, and the patient’s overall condition (Thilander et al., 1999; Oesterle et al., 2000). Similarly, loading protocols can be conventional, early, or immediate. Immediate loading offers the advantage of reduced treatment time and improved patient comfort, provided that adequate primary stability is achieved and micromovement is controlled (Weber et al., 2009; Gallucci et al., 2014). Transitional prostheses may also play an important role during healing by allowing soft tissue conditioning and progressive refinement of the emergence profile while maintaining function and esthetics (additional clinical considerations regarding immediate restoration and loading are discussed in the ITI Academy module on Immediate Restoration and Loading, Bechelli, n.d.).
Beyond technical considerations, successful implant rehabilitation depends heavily on understanding and managing patient expectations. Contemporary patient-centered care encourages active participation in treatment decisions, making preoperative communication essential (Yao et al., 2014; Crow et al., 2002). Implant treatment outcomes are increasingly evaluated not only by survival rates but also by esthetics, comfort, function, longevity, and psychosocial aspects such as self-confidence and oral-health-related quality of life (Carr et al., 2011). However, exposure to marketing or inaccurate information may generate unrealistic expectations regarding esthetic perfection, treatment duration, or maintenance requirements (Rustemeyer et al., 2007; Omar et al., 2006). Therefore, clear discussion of treatment length, costs, potential limitations, and long-term maintenance is fundamental. Aligning achievable clinical outcomes with patient expectations through coordinated surgical and restorative planning ultimately enhances satisfaction and the perceived success of implant rehabilitation (Yao et al., 2014; Crow et al., 2002).
Clinical implications: Selecting the appropriate treatment approach requires balancing biological, technical, and patient-related factors, ensuring that surgical and restorative decisions align with realistic expectations, treatment timelines, and long-term functional and esthetic goals.thetic goals.
Conclusion
Successful implant therapy relies on the seamless integration of surgical and prosthetic planning, guided by both clinical principles and patient-centered goals. Decisions made during prosthetic planning directly influence surgical complexity, while surgical choices can either limit or facilitate prosthetic rehabilitation. When these phases are approached in isolation, the risk of technical complications, biological issues, and patient dissatisfaction increases.
By adopting a collaborative, interdisciplinary approach, clinicians can optimize implant positioning, prosthetic design, and soft tissue management, ultimately improving functional outcomes, esthetics, and long-term predictability. A practical understanding of the dynamic interaction between prosthetic and surgical decisions not only streamlines daily practice workflow but also enhances patient experience, reduces treatment morbidity, and supports more efficient, cost-effective care.
Incorporating these insights into routine implant practice underscores the importance of viewing implant therapy as a holistic process rather than a sequence of isolated steps. Such an approach ensures that each treatment decision contributes to overall clinical success and patient satisfaction.
_____________________________________________________________________________
This article was developed during my ITI Scholarship at the School of Dental Medicine, University at Buffalo, under the mentorship of Dr. Ahmet Orgev, Clinical Director of the Buhite-DiMino Implant Center and Dr. Cui Cui, Assistant Professor in the Department of Restorative Dentistry, who provided valuable guidance in the preparation and review of this article as part of my ITI Scholarship experience.






