
Introduction
In recent years, rapid developments in digital technology have brought about changes in various fields. Advanced technologies such as artificial intelligence (AI) and robots have also been introduced into the medical field, and the trend is similarly widespread in the field of dentistry.

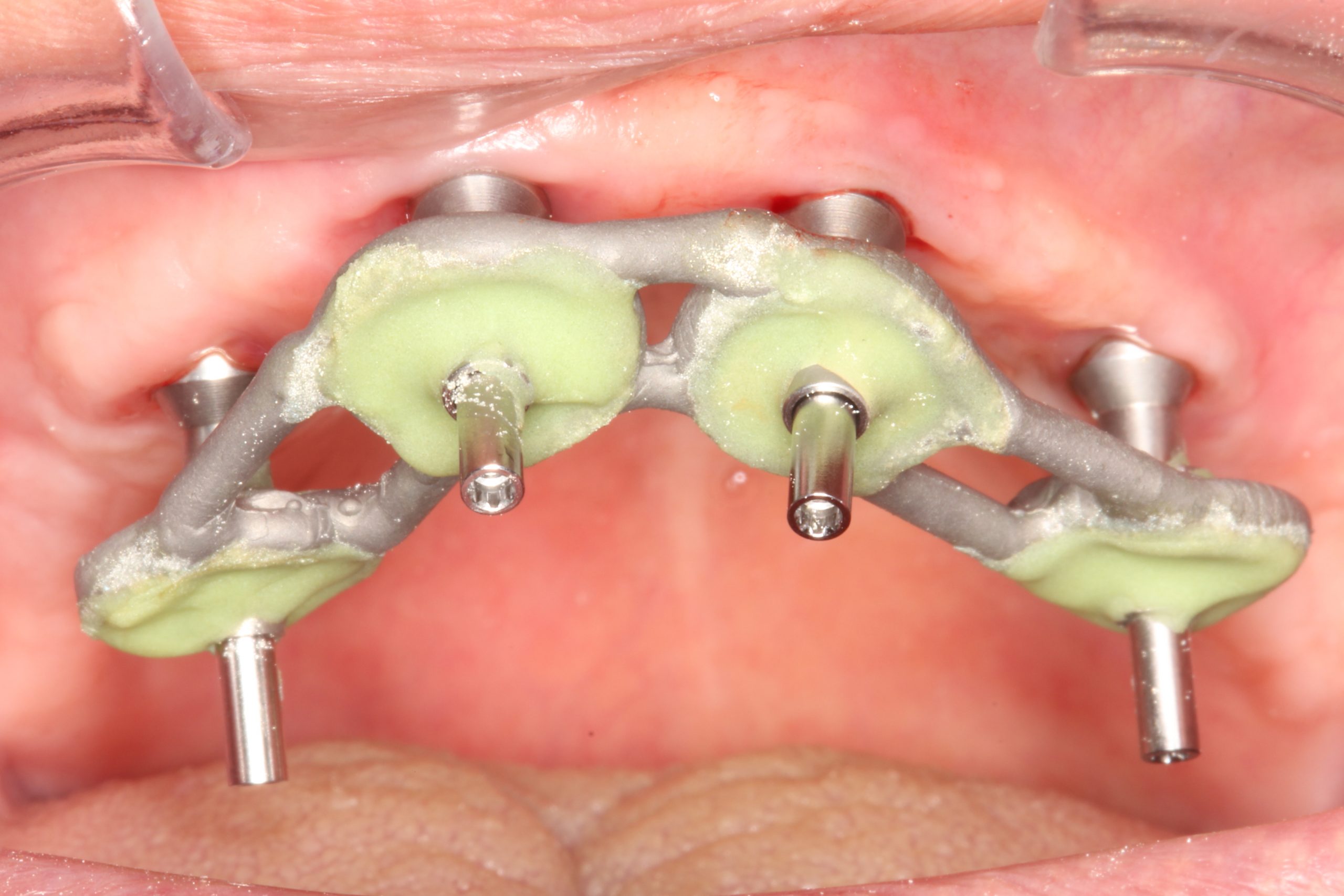
The intraoral scanner is a handheld device with a small optical camera (Fig. 1) that is widely used in dental implant treatment for the acquisition of virtual dental models (Michelinakis et al. 2021). Implant-supported prosthodontic restorations require a high degree of accuracy of a virtual dental model. Currently, the accuracy of digital impressions is comparable to conventional impressions, although the open-tray splinted impression technique is still considered clinically to be the gold standard for full-arch implant restorations (Papaspyridakos et al. 2020) (Figs 2 – 3). However, intraoral scanners have a lot of advantages for clinicians and patients. Hence, the objective of this article is to introduce the clinical applications and advantages of intraoral scanners in implant treatment.

The advantages of intraoral scanners
The advantages of the intraoral scanner as part of implant treatment include:
- Potential cost- and time-effectiveness
Since digital impression techniques are faster and don’t require dental impression materials and dental cast models, they can shorten the chair-side time and save on dental materials in the dental office and the laboratory. - Reducing the distortion of impression materials
Impressions can become deformed, which affects the fit of the restoration. Impressions are poured in dental stone, but inaccuracies can occur in the production of dental cast models as well. By using intraoral scanners, it is possible for us to avoid distortion from the impression and gypsum materials. - Taking an impression before completion of osseointegration
Since conventional impression materials are not used for intraoral scans, it is possible to take an optical impression during surgery with a low risk of contamination of the surgical field. In addition, intraoral scanners make it possible to take an impression during the early stages of osseointegration without stressing the implant abutment component (Lee et al. 2013). - More comfortable for patients with a sensitive gag reflex and profuse salivation
Digital impression techniques can reduce foreign object sensation and breathing difficulties. In addition, impression materials need a setting time of about four minutes. Hence, digital impressions can be taken more comfortably than conventional impressions for patients (Yuzbasioglu et al. 2014). - Immediate evaluation of impressions and partial re-impression possible in the dentist’s chair
Intraoral scanners can immediately reconstruct the scanned image on the monitor, and the area where scanning is insufficient is marked clearly. In this case, it is possible to reproduce the area that was poorly scanned without losing all the impression data as with the conventional method. - Easier to store and transfer digital images between the dental office and the laboratory
Since the impression is stored as digital data, it is not necessary to store multiple dental cast models, which is excellent in terms of storage period and space. Transfer between the dental office and the dental laboratory is easier and faster.
Conventional prosthodontic treatment in bone-level implant treatment
In the treatment sequence for bone-level implant treatment, the implant is placed following examination and diagnosis including CBCT and surgical treatment planning. After osseointegration, the implant is exposed, and the healing abutment is placed at the time of re-entry. To achieve optimal esthetic results and access to oral hygiene, it is critical to create the mucosal contours in the transition zone with the provisional restoration or a customized healing abutment. Since the peri-implant mucosa collapse immediately after the restoration is removed, transferring the shape of the provisional restoration to the impression coping allows for ideal final restoration contours (Figs 4 – 5).


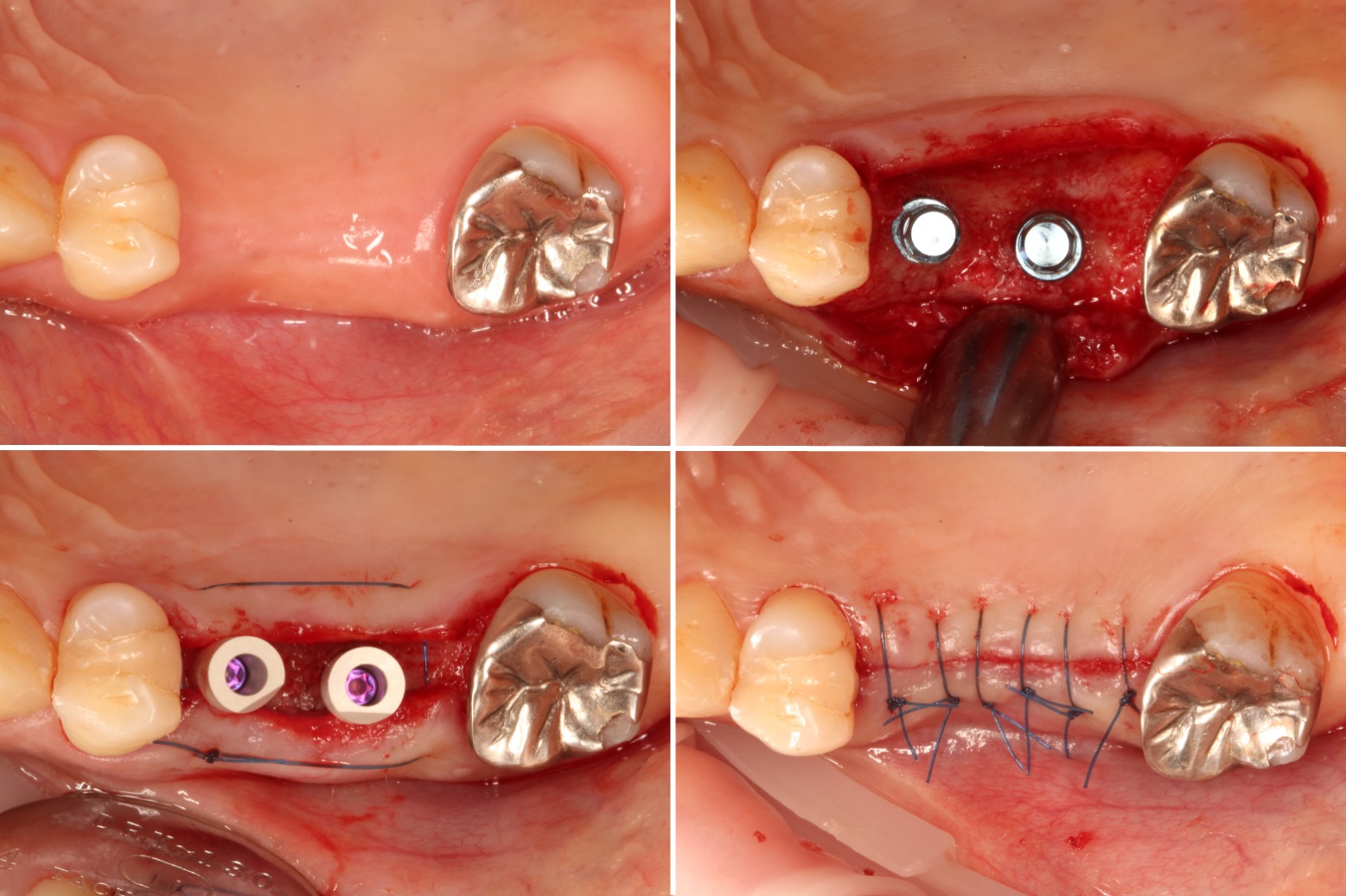
The clinical application of IOS scans with simultaneous implant placement
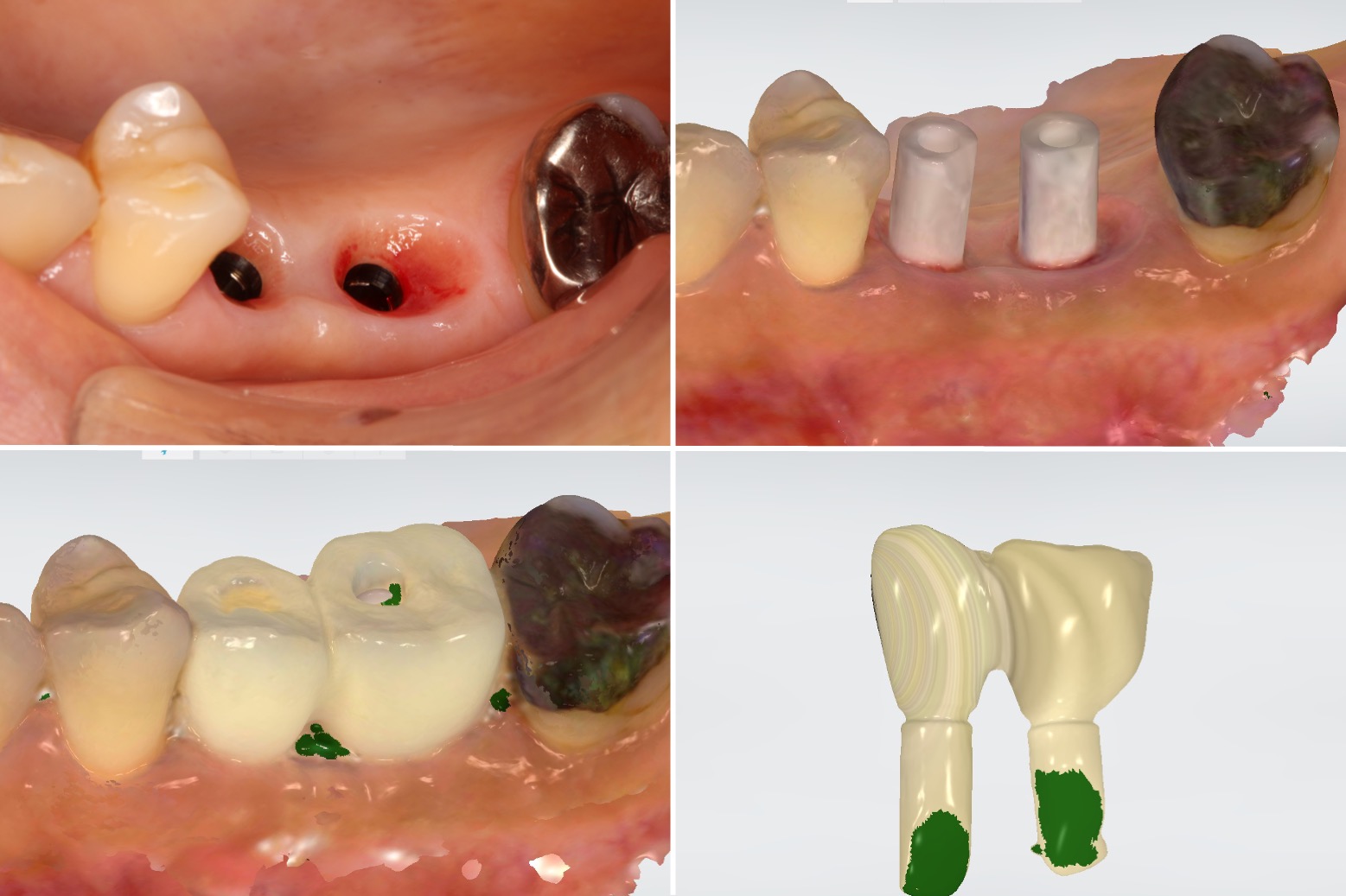
As described above, it is necessary to adjust the emergence profile of the provisional restoration or use a customized healing abutment to create ideal mucosal contours in submerged bone-level implant treatment. With the conventional impression method, there is a risk of inflammation and contamination in the surgical area due to residual impression material if the impression is taken at the same time as implant placement. However, intraoral scanners allow for a reduction in risk, and the impression for the provisional restoration can be taken immediately after implant placement (Figs 6 – 7).

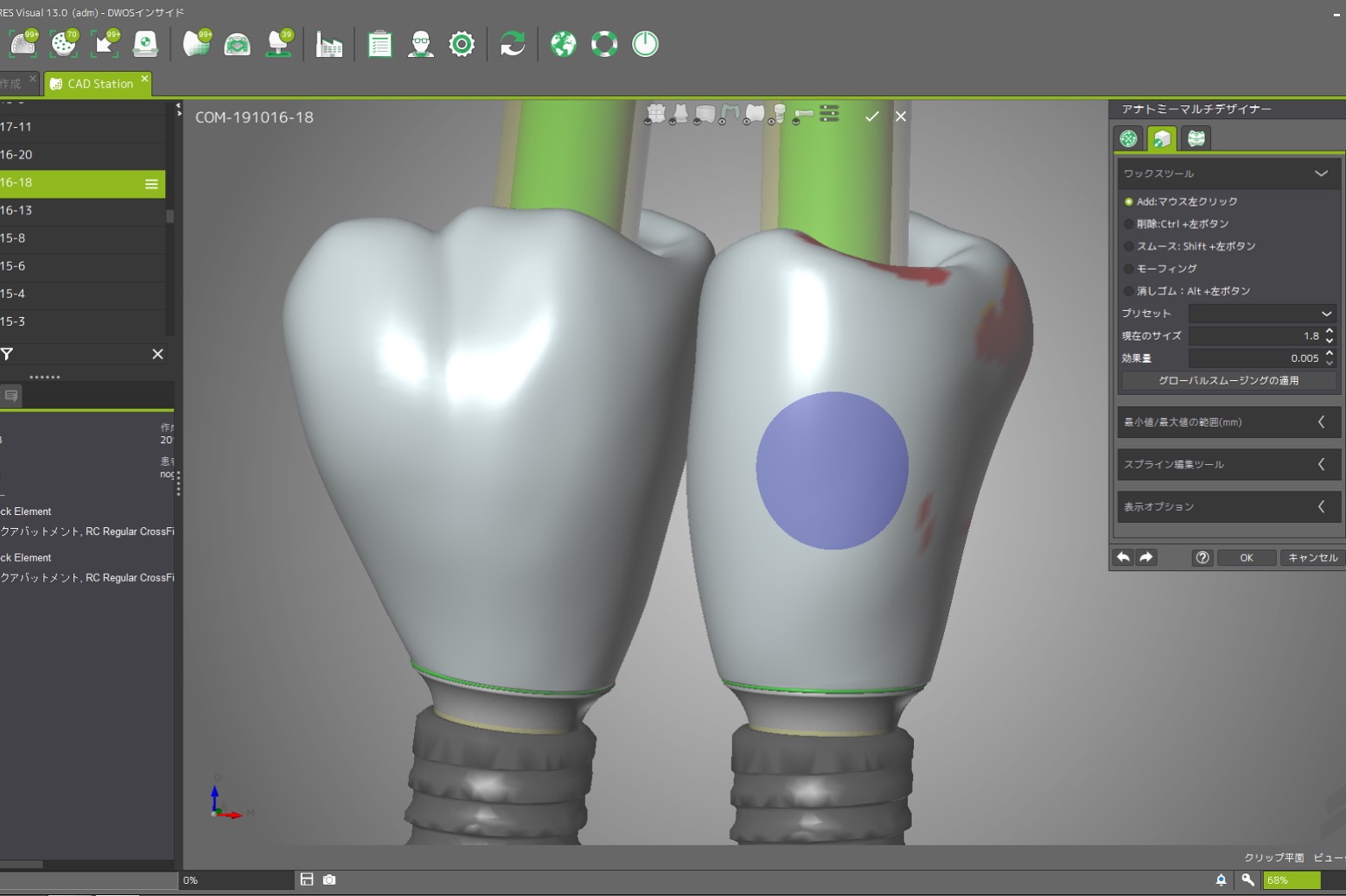
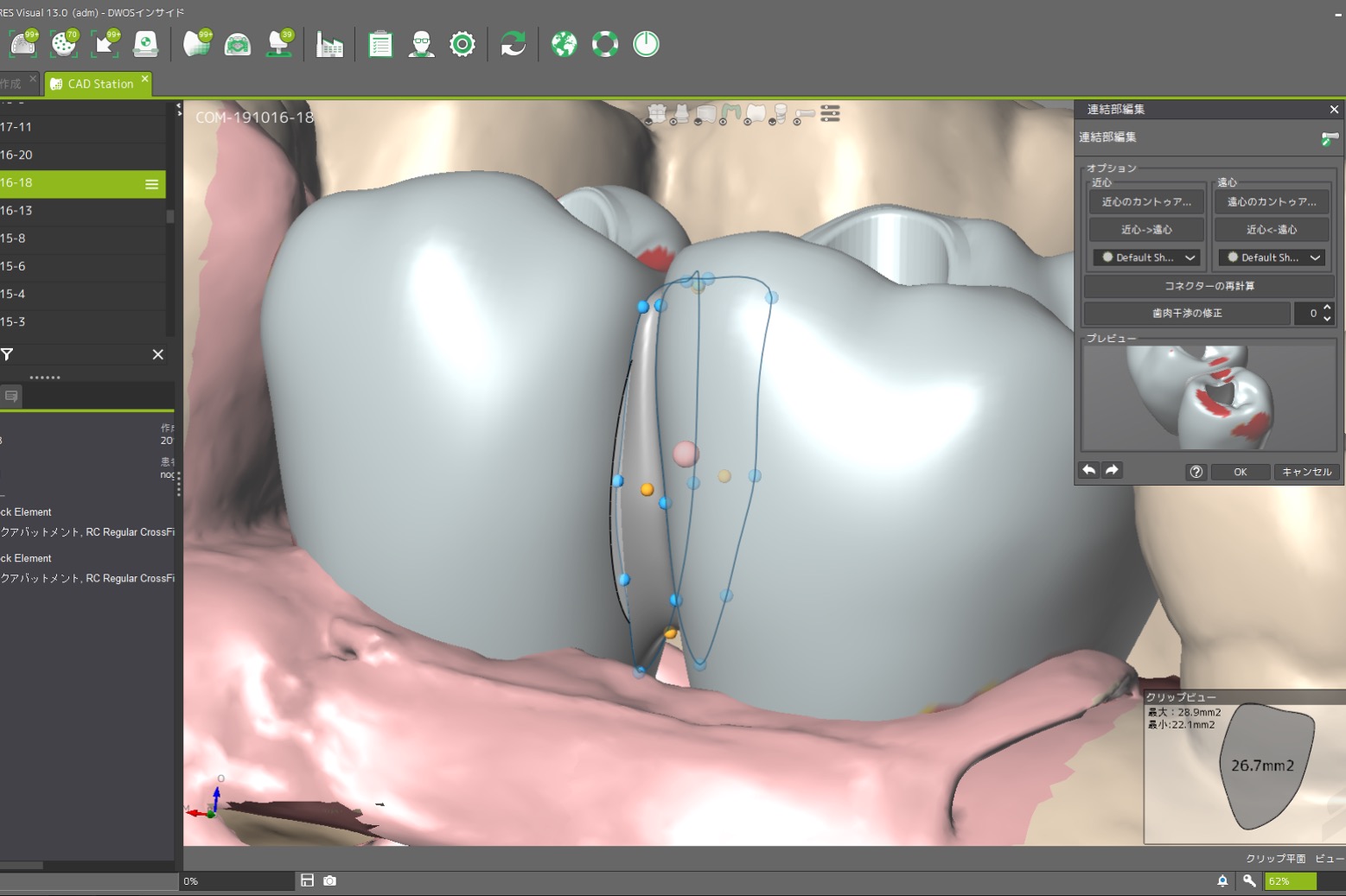
Therefore, this technique can make the contours directly by delivering the provisional restoration with an ideal emergence profile at the time of re-entry after successful osseointegration in a submerged approach (Figs 8 – 10).

It is then possible to wait for soft tissue maturation and duplicate the emergence contour established in the provisional restoration for the final restoration. After soft tissue maturation, the whole dentition and the surrounding mucosa are scanned. Then, the provisional restoration is gently removed and scanned extraorally to accurately replicate and transfer the emergence profile for the final restoration (Sasada et al. 2020) (Figs 11 – 13).


Abutment disconnection and reconnection significantly affect peri-implant marginal bone levels (Koutouzis et al. 2017). Hence, it can be considered that this treatment protocol has a great advantage in that the number of times that the abutment is disconnected and reconnected can be reduced substantially.
Conclusion
As described in this article, intraoral scanners seem to be useful for implant treatment, but the open-tray splinted impression technique is still considered clinically the current standard technique for full-arch implant restoration (Papaspyridakos et al. 2022). However, a digital approach to full-arch implant restoration will become possible in the near future since digital technology is making continuous rapid progress. On the other hand, it is necessary for clinicians to thoroughly examine the information before jumping into the newly created technology. With the further evolution of digital technology in the future, it is expected that new possibilities for digital dentistry will open up.




