Introduction
The “hidden” changes in implant dentistry:
In daily practice, we mostly rely on what we can see clinically or what appears calcified on radiographs. The true “black box” of implant dentistry, however, is the softtissue interface. Conventional tools often fail to capture the early biological dynamics of softtissue integration, subtle inflammatory changes, or their real-time resolution. Intraoral ultrasonography (IUS) offers a noninvasive, radiation-free window into peri-implant healing, allowing quantitative assessment of mucosal thickness and vascularity in real time.
The predictability of dental implants is no longer defined solely by osseointegration but by the long-term stability of the peri-implant phenotype (Alrmali et al., 2026; Adell et al., 1986; Berglundh et al., 1991; Di Gianfilippo et al., 2020). While periapical radiographs and CBCT remain the gold standard for evaluating hard tissue, they provide limited information on supracrestal tissue adhesion (STA), the biological seal that protects the bone-implant interface (Adell et al., 1986; Berglundh et al., 1991; Chan et al., 2017; Strauss et al., 2024). Traditional soft-tissue assessment relies on visual inspection and manual probing, which are subjective and cannot quantify internal changes such as mucosal thickness (MT) or vascular perfusion (Sabri et al., 2025). IUS fills this diagnostic gap. As a noninvasive, radiation-free modality, it uses high-frequency sound waves (up to 20 MHz) to generate real-time, high-definition cross-sectional images of both soft and hard peri-implant structures (Chan et al., 2017; Strauss et al., 2024; Eger et al., 1996).
Before presenting the detailed clinical cases, it is important to emphasize the role of a stable mucosal seal within the MICH concept for long-term hard- and soft-tissue stability (Alrmali et al., 2026). In Figures 1–3, the patient has maintained implants placed in 2001; tooth #19 received a free gingival graft, and despite a suboptimal prosthetic design for #14, the 2015–2025 radiographs show minimal change (Figures 2B and 2C). In addition, vascular mapping with color Doppler was used to evaluate blood flow around implant #4, demonstrating a robust vascular supply helps justify simultaneous procedures and provides a baseline for monitoring subsequent graft integration.
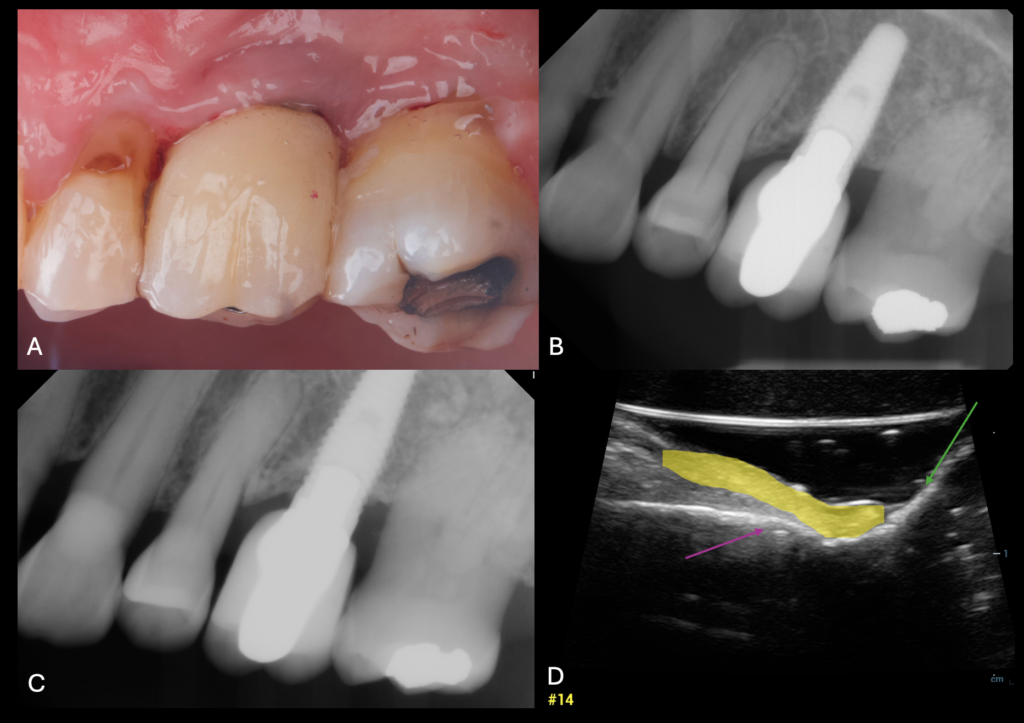
Figure 2. Same patient at figure 1 and despite the prosthetic design still the mucosal seal represents a shield against bacterial invasion. Compromised soft‑tissue phenotype around posterior fixed prostheses. A: Clinical view showing thick, keratinized mucosa but with limited interproximal access. B, C: Periapical radiographs demonstrating stable crestal bone levels over 10 years. D: IUS cross‑section with highlighted mucosal thickness (yellow) and implant surface (purple arrow) confirming a thick soft‑tissue seal around tissue level implant. 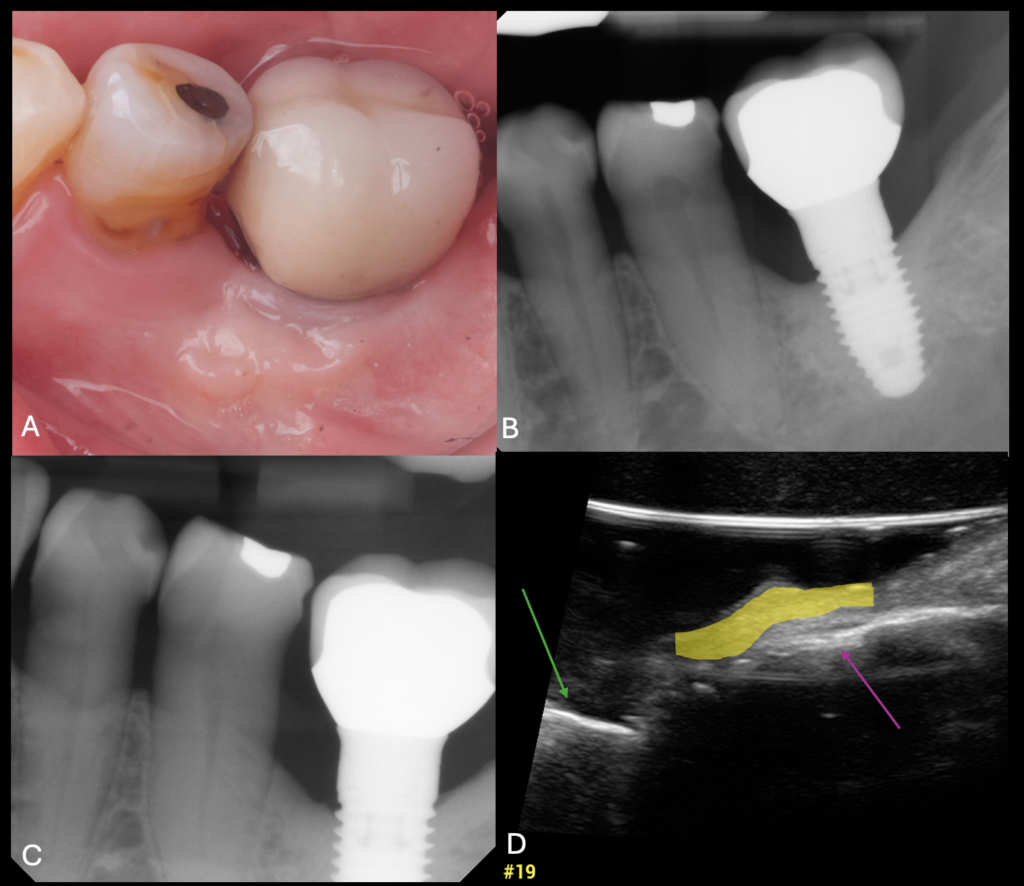
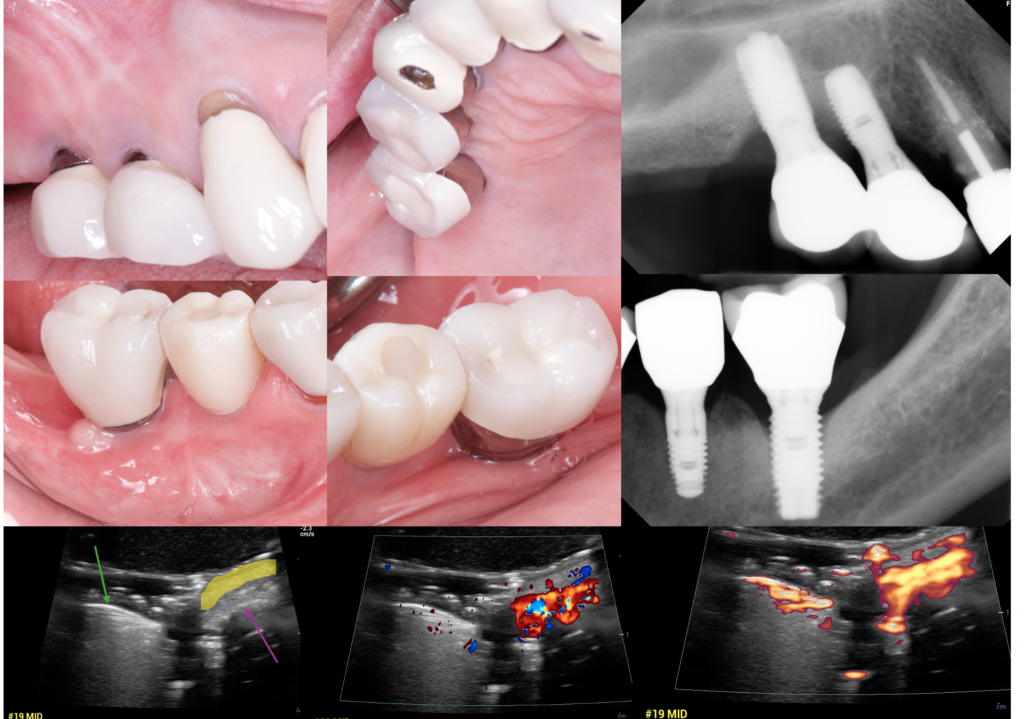
Figure 3. Long‑term stability of posterior implants placed under the MICH concept. A: Clinical photograph showing a 10‑year follow‑up with preserved soft‑tissue contours after free gingival graft. B, C: Baseline and 10‑year periapical radiographs demonstrating zero marginal bone changes. D: IUS B‑mode and Doppler images of the #19 implant showing adequate mucosal thickness (yellow) and rich vascularization surrounding a stable bone crest. 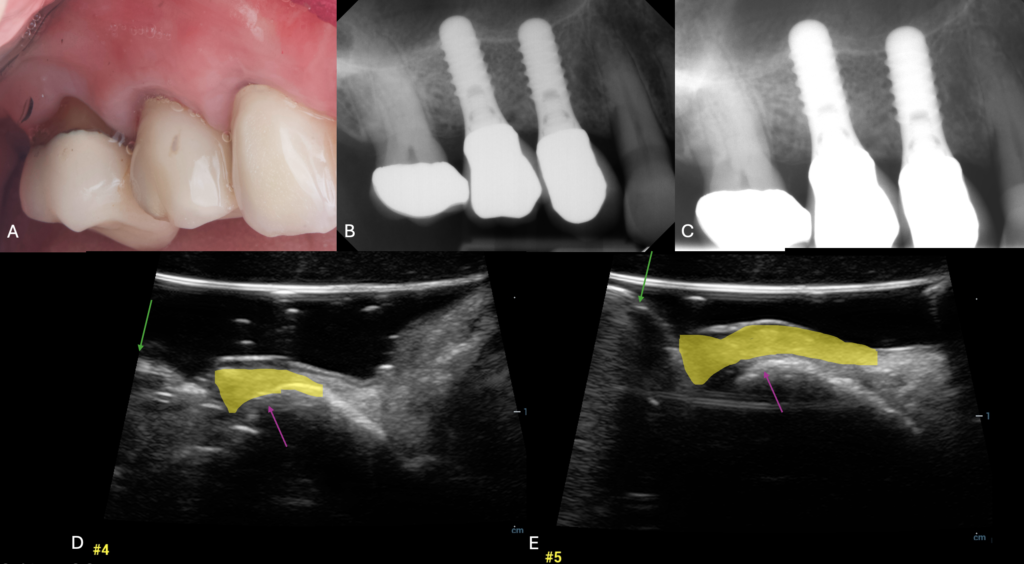
Figure 1. Clinical and radiographic appearance of a posterior implant restored under the MICH concept with stable peri‑implant phenotype. A: Intraoral views showing healthy keratinized mucosa. B, C: Periapical radiographs demonstrating stable crestal bone levels over 10 years. D, E: Intraoral ultrasonography (IUS) B‑mode and color Doppler images illustrating adequate mucosal thickness and supracrestal soft‑tissue complex around the implant.
A Case-Based Journey
Part I: Application in soft–tissue augmentation around dental implants:
Soft-tissue augmentation around implants aims to increase mucosal thickness, enhance peri-implant tissue stability, and improve esthetic integration. Long-term success depends not only on initial volume gain but also on the stability of augmented tissues over time (GalarragaVinueza et al., 2024; Tavelli et al., 2021; Strauss et al., 2024; Wang et al., 2025).
Intraoral US can help clinicians to:
• Quantify peri-implant mucosal thickness before and after augmentation.
• Track volumetric stability and remodeling of augmented tissues.
• Differentiate transient postoperative edema from true soft tissue gain.
• Perform repeated measurements without mechanical trauma to the site.
The narrative review by Strauss et al. highlights that ultrasound is particularly valuable during early healing, when conventional probing is contraindicated, enabling longitudinal insight into tissue maturation and stabilization that is difficult to capture clinically (Strauss et al., 2024).
1. Esthetic Zone Management: Immediate (IIP) vs. Delayed (DIP) Placement:
IIP Case Monitoring: High-resolution IUS was employed to track both hard- and soft-tissue healing following immediate implant placement and connective tissue grafting. This allowed for a noninvasive longitudinal assessment of buccal plate thickness and mucosal volume changes over time (Figure 4).
DIP and Papilla Assessment: In delayed placement scenarios, IUS was utilized post-soft-tissue conditioning with provisional crowns. The modality enabled a detailed three-dimensional evaluation of the height and thickness of the inter-implant papilla, complementing traditional clinical photography and indices.
The Role of Vascular Mapping:
Augmentation procedures, such as those performed for Seibert Class III ridge defects, rely heavily on the recipient site’s biological capacity.
• Presurgical vascular assessment: Color Doppler assessment was used to quantify baseline blood flow within the buccal mucosa. Identifying a relatively robust vascular supply in the graft recipient area helped justify the decision for simultaneous softtissue augmentation (GalarragaVinueza et al., 2024; Tavelli et al., 2021; Chan et al., 2020).
• Longitudinal tracking: IUS enables clinicians to quantify peri-implant mucosal thickness both before and after augmentation, providing a baseline for comparison during long-term follow-up.
Device description and imaging settings:
Intraoral ultrasonography was performed with a high-frequency linear transducer specifically adapted for intraoral use (frequency range 10–20 MHz, footprint approximately 10–15 mm). The probe was connected to a portable ultrasound unit capable of B-mode, color Doppler, and power Doppler imaging. For softtissue visualization, B-mode scans were acquired at 15–18 MHz with a shallow depth setting (10–15 mm) and tissue harmonic imaging activated to enhance boundary definition between mucosa, periosteum, and implant surface. Color Doppler and power Doppler assessments of periimplant perfusion were performed using a pulse-repetition frequency between 0.7 and 1.0 kHz and low wall-filter settings to detect slow capillary flow while avoiding motion artefacts from probe handling (Chan et al., 2017; Tavelli et al., 2021; Chan et al., 2020).
A generous layer of sterile aqueous gel was applied to the probe tip and covered with a disposable barrier to ensure acoustic coupling and infection control. The probe was positioned parallel to the long axis of the implant for sagittal scans and perpendicular for transverse scans, using adjacent teeth and the prosthetic crown as orientation landmarks. Gain and time-gain compensation were standardized at the beginning of each session and kept constant for serial follow-up to permit comparison of measurements over time (Chan et al., 2017; Tavelli et al., 2021).
Practical clinical application guidelines:
In routine practice, we recommend using intraoral ultrasonography at three key time points:
• Baseline (pre-surgical or pre-augmentation): Record mucosal thickness at the mid-facial, interproximal, and palatal/lingual sites, and obtain color Doppler images to document baseline perfusion at the intended graft or peri-implantitis surgery site.
• Early healing (2–4 weeks): Repeat B-mode scans to distinguish transient postoperative edema (diffuse, hypoechoic thickening with increased Doppler signal) from organized softtissue gain (more homogeneous echogenicity and regular contours), particularly when probing is contraindicated.
• Medium-term follow-up (3–6 months and beyond): Use standardized sagittal scans through the implant midline to monitor supracrestal softtissue height and facial mucosal thickness; stable or increasing values with a homogeneous vascular pattern suggest favorable remodeling, whereas thinning or irregular contours may indicate risk for future recession or peri-implantitis (Thoma et al., 2009; Schwarz et al., 2018; Tomasi et al., 2016; Renvert & Polyzois, 2018; Jepsen et al., 2015).
For reproducible measurements, the probe should be stabilized on adjacent teeth or the prosthetic crown, with images captured at the same angulation and reference points at each visit. Measurements of mucosal thickness and supracrestal softtissue height can then be made directly on the frozen images using the device’s caliper tools, ideally averaged over three consecutive scans to minimize operator variability.
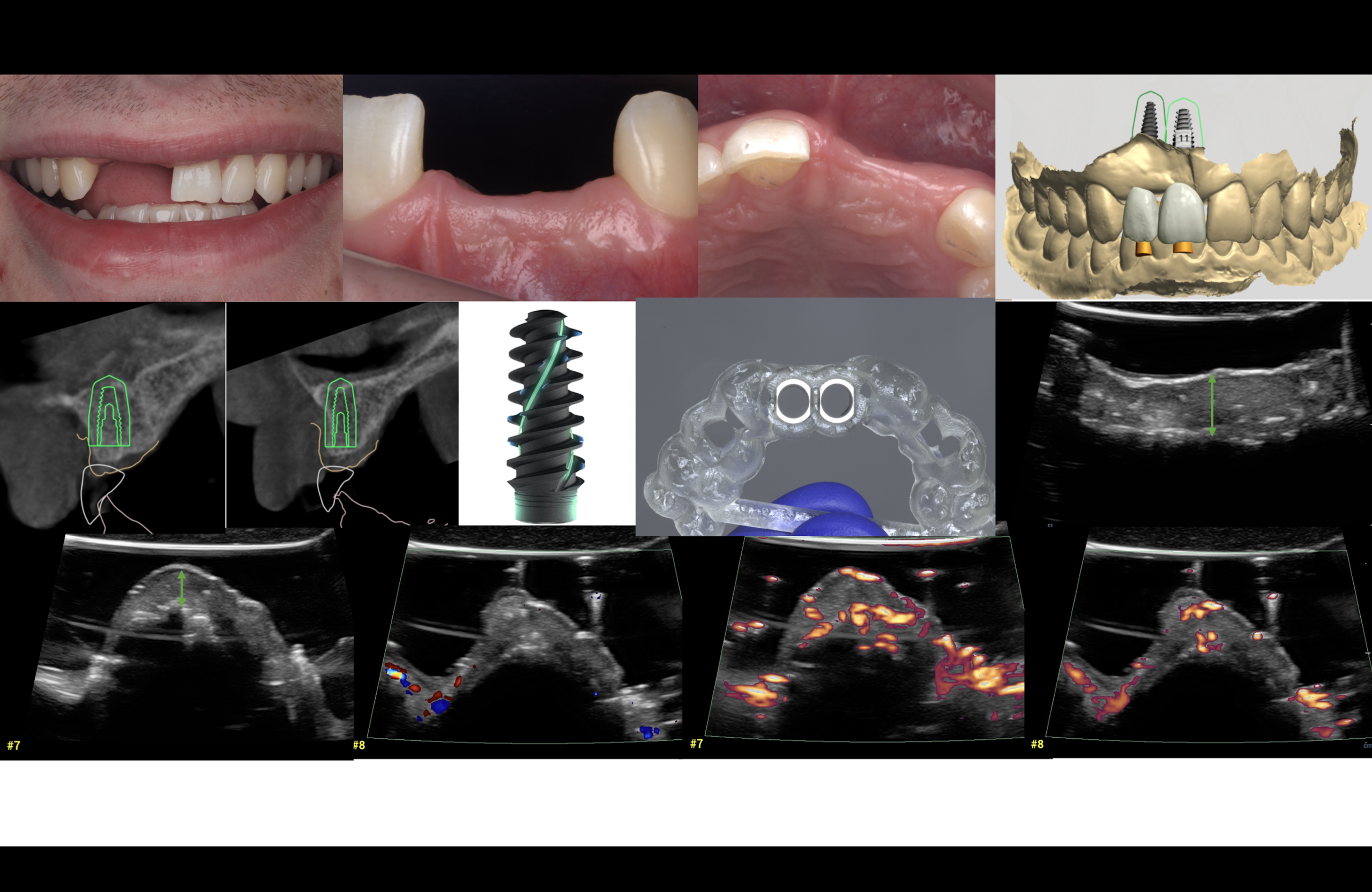
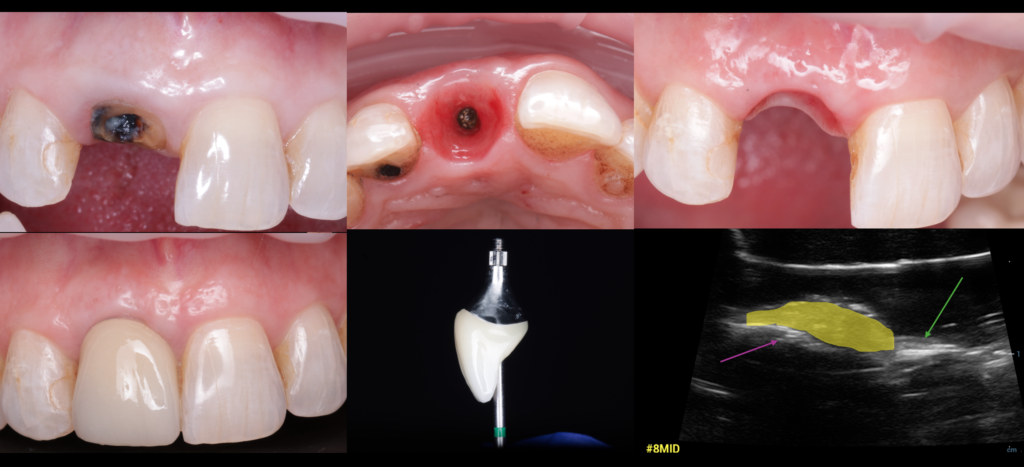
Case presentation:
A 23yearold systemically healthy male with a history of trauma and loss of the maxillary right lateral and central incisors (#7 and #8) presented with esthetic concerns and a localized anterior ridge defect. Radiographic and clinical examination confirmed a combined hard- and soft-tissue deficiency compatible with a Seibert Class III ridge deformity. Preoperative intraoral ultrasonography further demonstrated a thin buccal softtissue phenotype with reduced mucosal thickness over the edentulous #7–8 region, corroborating the clinical impression of an inadequate ridge volume (Figure 5).

This case report illustrates a simultaneous hard- and soft-tissue management approach designed to reconstruct the anterior maxillary ridge and create favorable conditions for an implantsupported restoration with an optimal esthetic outcome. The first-stage surgery consisted of simultaneous implant placement, guided bone regeneration, and vertical softtissue augmentation at the #7–8 site. Under local anesthesia, a full-thickness flap was elevated to expose the defect and allow prosthetically driven implant positioning. The buccal defect was augmented using a particulate cortical allograft mixed with autogenous bone and covered with a resorbable collagen membrane. A palatal connective tissue graft was then harvested and positioned over the implant crest beneath a tension-free coronally advanced flap to achieve at least 2–3 mm of vertical softtissue thickening. Flaps were sutured for complete primary closure, and the implants were left submerged for approximately 4 months before second-stage surgery and provisionalization (Figure 6).
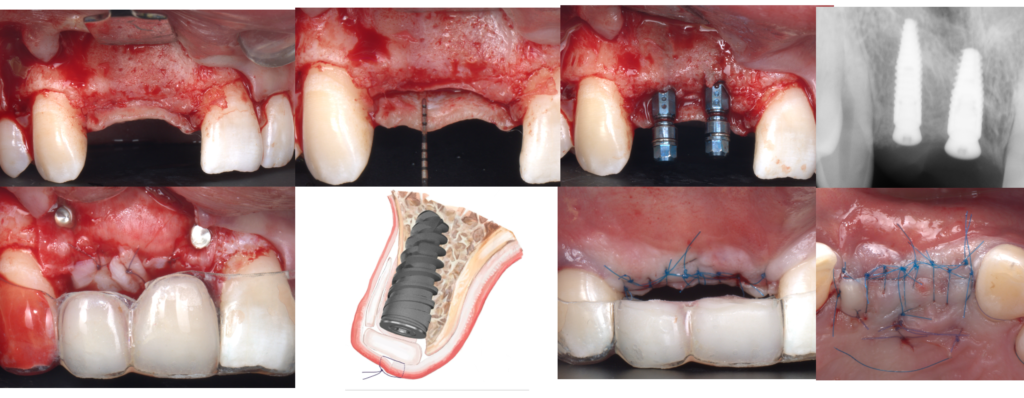
Surgical management of anterior peri‑implant defect #7,8 with simultaneous soft‑tissue and hard‑tissue augmentation. Intraoperative exposure of implants with thin buccal bone. Placement of particulate graft material and membrane adaptation over the defect and collagen membrane used for guided bone regeneration, CTG also was fixed over the crest to enhance vertical tissue height. Primary flap closure and immediate postoperative view demonstrating tension‑free soft‑tissue coverage.
Second-stage surgery included implant uncovery, buccal flap preparation, and placement of an inverted T-shaped palatal connective tissue graft to contour the buccal aspect and fill the inter-implant embrasure. Provisional screw-retained crowns were immediately connected and carefully contoured to provide gentle support for the grafted tissues, guiding papilla formation and shaping the emergence profile during healing. High-resolution intraoral ultrasonography was performed at multiple time points after both the first (implant placement + GBR + vertical softtissue augmentation) and second (inverted T-CTG) interventions, enabling noninvasive monitoring of buccal plate thickness and mucosal volume changes over time. At the final follow-up, following softtissue conditioning with provisional restorations, ultrasound imaging was also used to assess the height and thickness of the inter-implant papilla, complementing clinical indices and photographic documentation for three-dimensional papilla evaluation (Figure 7).
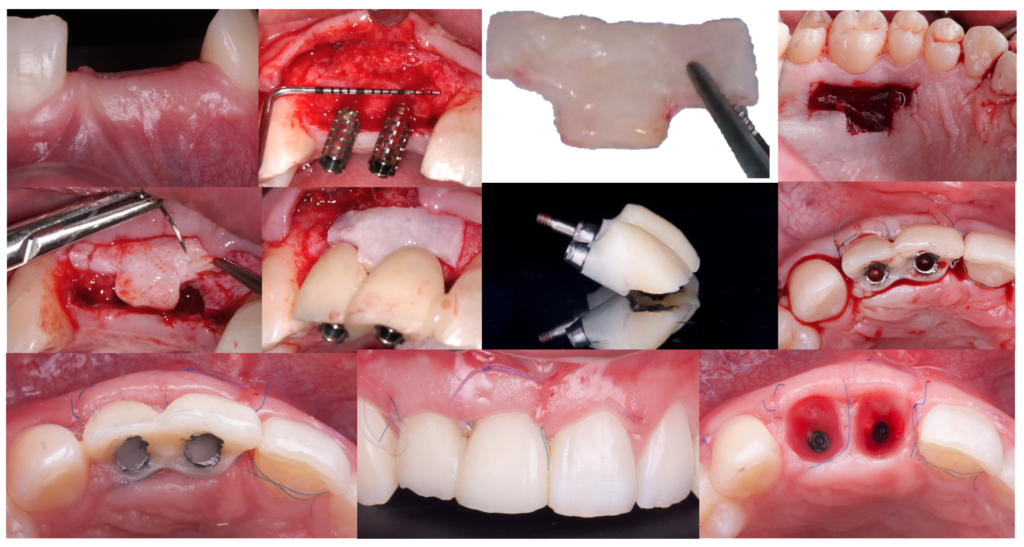
Surgical and prosthetic sequence for immediate implant placement at sites #7 and #8 with simultaneous buccal soft‑tissue augmentation utilizing inverted T-shaped CTG. The panels illustrate the adaptation of the screw‑retained provisional restoration to support the peri‑implant mucosa, and early postoperative views showing preservation of papillae and emergence profile around the provisional crowns.
Different ultrasound modes were applied to characterize softtissue dynamics at the grafted site. B-mode imaging was used to quantify buccal mucosal thickness and to document progressive softtissue gain over both implants (Figure 8). Color and power Doppler modes were additionally employed to visualize blood flow and early perfusion within the grafted area, revealing increased vascularization during the initial healing phase, consistent with successful integration of both the softtissue augmentation and the connective tissue grafts (Figure 9).
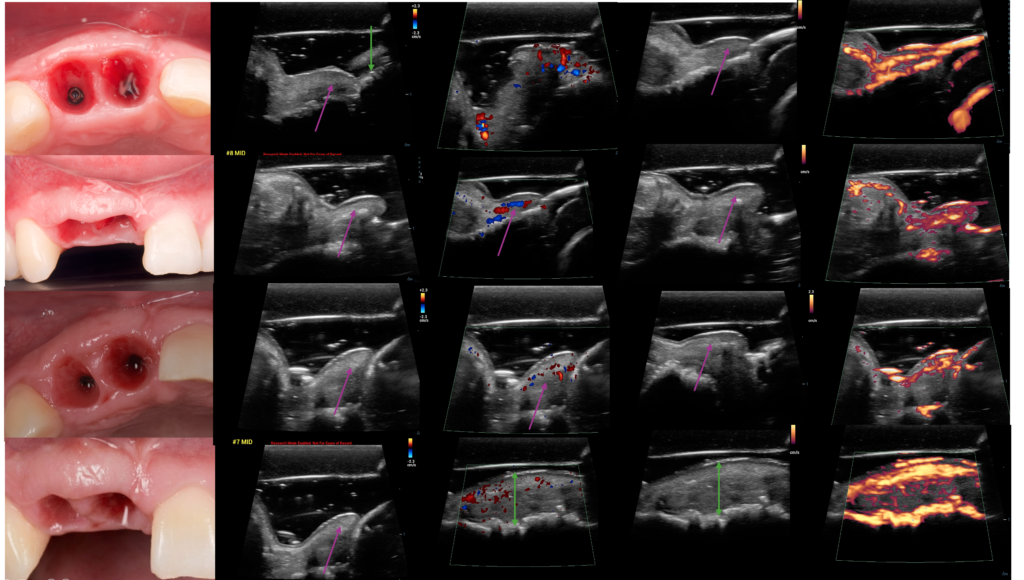
Immediate and early healing of anterior maxillary implants evaluated with IUS. Left column: Clinical views of extraction sockets and early soft‑tissue maturation at sites #7 and #8. Remaining panels: Serial IUS B‑mode and Doppler images at different time points showing progressive increase in mucosal thickness (green measurement bars) and development of an organized vascular network over the healing implant sites. 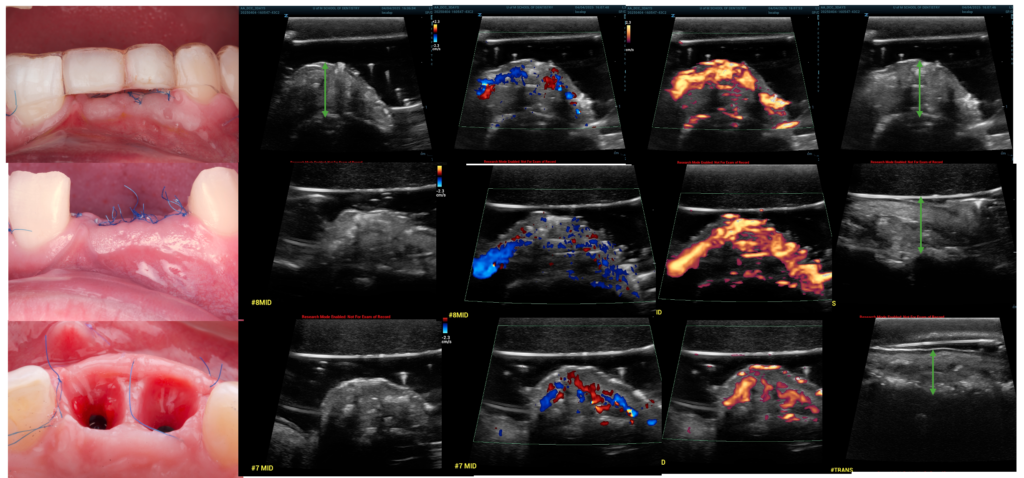
Color Doppler evaluation of peri‑implant vascularity at same implants. Follow‑up Doppler IUS demonstrating increased, more homogeneous blood‑flow signals within the supracrestal soft tissues after soft‑tissue conditioning. In addition, IUS B‑mode and color Doppler images at sites #7 and #8 showing progressive increase in mucosal thickness (green arrows) and an arch‑shaped band of vascular signals corresponding to the developing supracrestal tissue adhesion.
Part II: Monitoring Healing After Peri-Implantitis Surgery
Surgical treatment of peri-implantitis aims to control infection and re-establish stable peri-implant hard and soft tissues, with outcomes typically evaluated using bleeding on probing, suppuration, probing depth, and radiographic bone levels (Thoma et al., 2009; Schwarz et al., 2018; Tomasi et al., 2016; Renvert & Polyzois, 2018; Jepsen et al., 2015; Wang et al., 2025). However, these conventional parameters mainly capture surface inflammation and bone changes and therefore do not fully reflect subsurface soft-tissue healing dynamics or early alterations within the peri-implant mucosa.
Intraoral ultrasonography provides complementary information by visualizing changes in peri-implant mucosal thickness and morphology following surgery. Reduction of inflammatory edema and stabilization of soft-tissue dimensions can be monitored over time, potentially allowing earlier recognition of compromised healing before overt clinical signs occur. As emphasized by Strauss et al., ultrasound should enhance not replace conventional clinical and radiographic follow-up (Strauss et al., 2024).
Case presentation:
An 85-year-old systemically healthy female presented with discomfort, bleeding on brushing, and concern about progressive tissue recession around a mandibular implant-supported restoration. Clinical examination revealed deep peri-implant probing depths with bleeding and suppuration, along with pronounced softtissue inflammation and mucosal recession compatible with moderate to advanced peri-implantitis. Radiographic assessment demonstrated crater-like bone loss extending beyond the middle third of the implant length, confirming a combined hard- and soft-tissue defect (Figure 10).
Preoperative intraoral ultrasonography was performed to characterize the periimplant softtissue phenotype and defect morphology. Sagittal scans showed a thin peri-implant mucosa with reduced supracrestal softtissue height and irregular mucosal contours, while transverse views helped delineate the circumferential extent of the inflammatory swelling and the position of the residual buccal plate. These findings complemented the clinical and radiographic data, refining the diagnosis and aiding in the selection of a resective-regenerative surgical approach.
Surgical treatment consisted of peri-implant flap elevation, thorough debridement and decontamination of the implant surface, and defectoriented regenerative therapy using bone graft material and a resorbable membrane, followed by softtissue refinement with a coronally advanced flap to improve peri-implant mucosal thickness and coverage (Figure 11). Intraoral ultrasound was utilized at early and late postoperative visits to monitor softtissue healing, documenting progressive reduction in inflammatory edema, increased mucosal thickness, and gradual stabilization of the supracrestal softtissue height. Serial scans allowed noninvasive visualization of contour improvement and facilitated early detection of any areas with delayed healing, thereby supporting individualized maintenance and long-term peri-implant health in this elderly patient (Figures 12 and 13).

Figure 11. Continued. Surgical management of a posterior peri‑implantitis defect at sites #4, #5, and #19 with hard‑tissue augmentation. The sequence shows flap elevation and defect exposure, implantoplasty of the suprabony components at #4 and #5, placement of an acellular dermal matrix (ADM) without additional bone grafting, and immediate postoperative views demonstrating tension‑free primary closure around #4 and #5. Particulate graft material is then placed over the buccal defect at #19 and covered with a collagen membrane, with immediate postoperative views confirming tension‑free primary closure around #19. 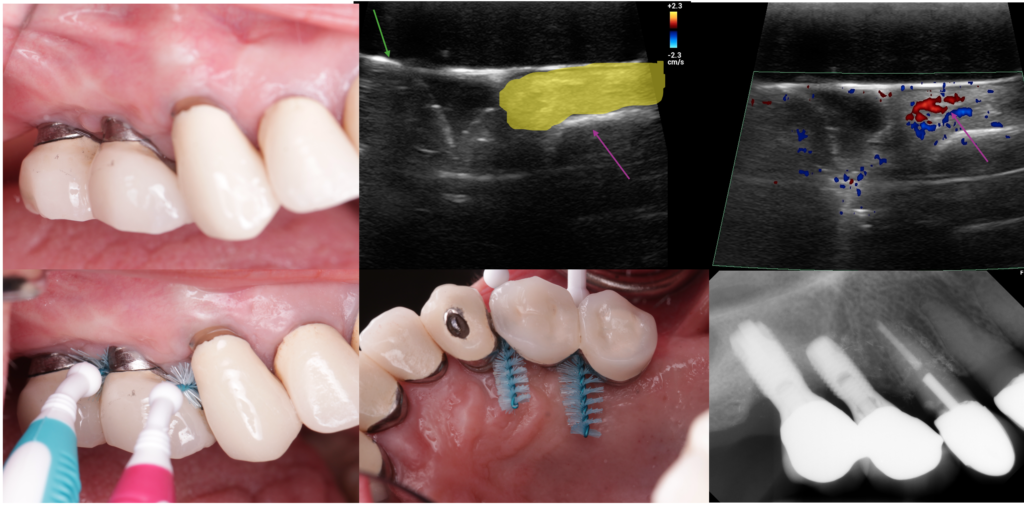
Figure 12. Six‑month clinical, radiographic, and IUS follow‑up after posterior implant restoration at sites #4 and #5 under the MICH concept. Buccal views show a stable, cleansable soft‑tissue contour with adequate interproximal access despite limited keratinized mucosa. IUS B‑mode image demonstrates increased mucosal thickness (yellow), and the color Doppler image reveals a well‑organized vascular network around the implant. Periapical radiograph confirms maintained crestal bone levels around implants #4 and #5. 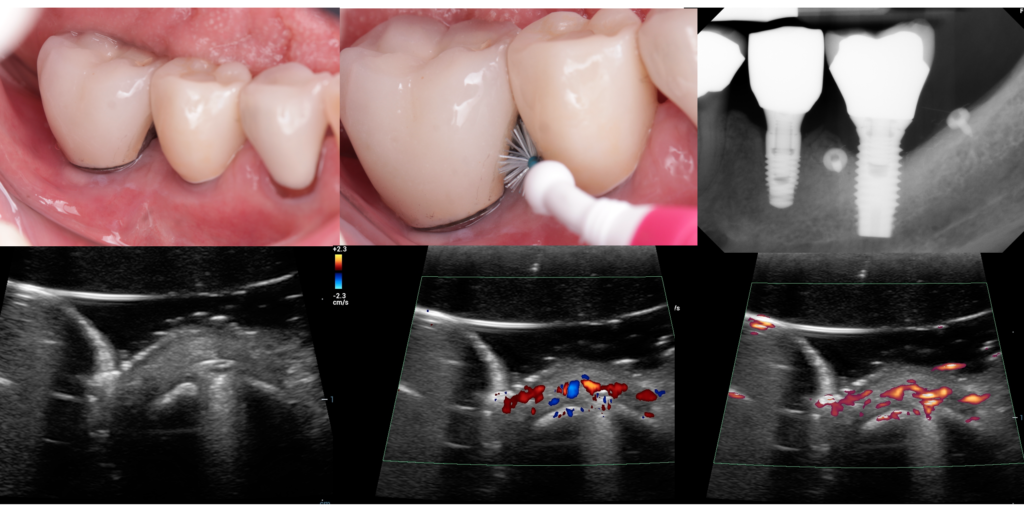
Figure 13. Six‑month clinical, radiographic, and IUS follow‑up after posterior implant restoration at site #19 under the MICH concept. Buccal views show a stable, cleansable soft‑tissue contour with adequate interproximal access despite limited keratinized mucosa. Periapical radiograph confirms maintained crestal bone levels around implant #19. IUS B‑mode image demonstrates increased mucosal thickness (yellow), and the color Doppler image reveals a well‑organized vascular network around the implant.
Part III: Current Limitations, Need for Standardization, and Future Perspectives:
Despite its promise, intraoral US has limitations. Image acquisition and interpretation are operator dependent, requiring specific training and standardized protocols to ensure consistent probe positioning and reproducible measurements. Limited penetration depth confines visualization primarily to superficial soft tissues, and universally accepted peri-implant ultrasound assessment protocols are still under development. As ultrasound hardware and dedicated intraoral probes continue to evolve, intraoral US is likely to assume a growing role in peri-implant soft-tissue diagnosis and longitudinal monitoring. Future research should focus on standardized imaging workflows, validation of diagnostic thresholds, and integration of ultrasound data into digital planning and maintenance protocols for soft-tissue augmentation and peri-implantitis management. Such developments may ultimately support more precise, minimally invasive, and data-driven peri-implant care.
Part IV: Clinical Significance
The integration of high-resolution intraoral ultrasonography (IUS) into the monitoring of these complex cases demonstrates a paradigm shift in how we evaluate peri-implant health and surgical outcomes. By providing real-time, cross-sectional imaging, IUS addresses several critical limitations of conventional clinical and radiographic techniques including:
• Objective quantification: IUS moves beyond subjective biotype classification to provide precise, millimeter-level measurements of mucosal thickness and supracrestal soft-tissue height.
• Longitudinal stability tracking: The modality is exceptionally suited for repeated follow-up examinations during wound healing and long-term maintenance because it is free of ionizing radiation.
• Biological differentiation: In augmentation and peri-implantitis cases, IUS allows the clinician to distinguish between transient postoperative edema and true biological soft-tissue gain, providing more accurate prognostic data.
• Enhanced reproducibility: When standardized scanning protocols are applied, IUS measurements demonstrate high reproducibility, supporting its utility in both private practice and clinical research settings.
Conclusion:
The future of implant dentistry lies in our ability to proactively manage the peri-implant phenotype rather than reactively treating disease. As demonstrated in these cases ranging from immediate esthetic placement to the resolution of peri-implantitis IUS provides a non-invasive “window” into the early biological dynamics of soft-tissue integration and inflammation resolution. As the ITI community continues to champion evidence-based excellence, the adoption of intraoral ultrasonography stands as a vital bridge between surgical intuition and measurable, reproducible success. By making the “hidden” visible, we can ensure the long-term functional and esthetic integrity of the restorations we provide for our patients.
Acknowledgements:
The author gratefully acknowledges Dr. Hamoun Sabri for his invaluable assistance with intraoral ultrasonography image acquisition for this study.




