Introduction
Building upon the foundational framework established in the previous review Registration Methods in Fully and Partially Edentulous Patients for Dynamic-Navigation-Assisted Implant Placement, Part I: Marker-Based Registration Techniques concerning the registration techniques utilized in dynamic-navigation-assisted implant placement, this subsequent discussion delves into the intricate domain of registration methodologies, particularly focusing on markerless registration techniques. Within the realm of dynamic navigation for dental implantation, especially in partially and fully edentulous cohorts, the integration of markerless registration signifies a significant paradigm shift. By opting for advanced imaging modalities and algorithmic computations over traditional physical markers, these methodologies not only drive a revolution in accuracy and efficiency but also epitomize a pivotal moment in implant dentistry. This review aims to elucidate the complexities and implications of markerless registration, shedding light on its transformative potential in enhancing patient outcomes within the field of dental implantology.
What are the frequently used markerless registration method in edentulous patients?
Marker fusion (MF) technique
This refers to a novel registration method that eliminates the need for artificial fiducial markers and stents in CBCT scans. Instead, high-contrast landmarks like teeth, implants, or abutments are used for registration, streamlining the workflow, and reducing errors. This technique was introduced as an innovative approach for registration and has been found to have comparable accuracy to other techniques, such as the use of GP markers and the fully radiopaque barium sulphate scan appliance (Ekram et al. 2022).
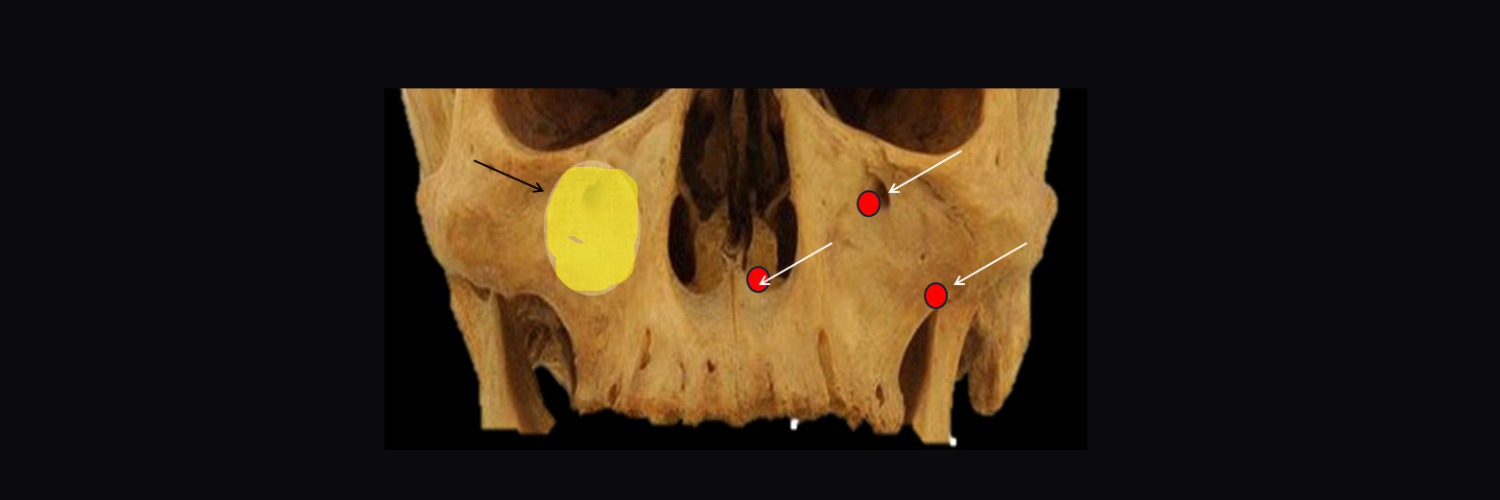
It can be point-based using anatomical landmarks like tooth cups, bony prominences, foramen etc. and surface-based like surface-matching method using a portable 3D scanner, laser surface scanning, surface scanning camera, video, and computer vision (Ekram et al. 2022, Fan et al. 2014) (Fig. 1).
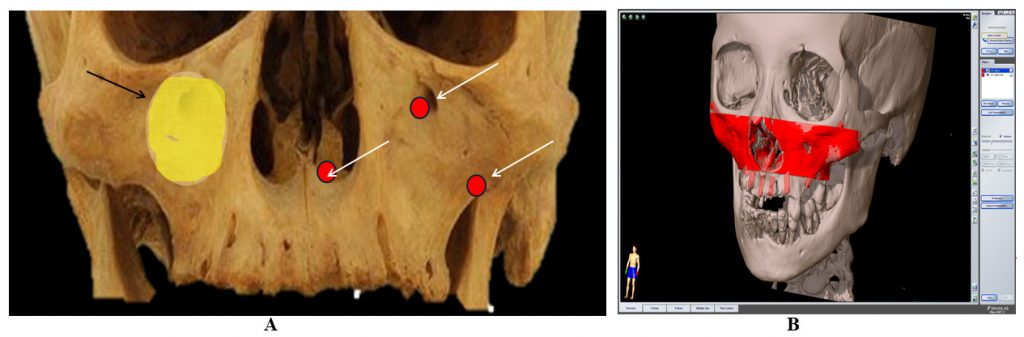
Fig. 1: Surface registration method. A: Three-point registration method was used for the bony landmarks: lateral nasal aperture, infraorbital foramen and inferior zygomaticomaxillary suture on the same side and maxillary sinus anterior wall area; B: STL image generated by converting the CT data used for surface registration
What are the advantages and disadvantages of markerless registration?
Markerless registration for fully edentulous patients has several advantages and disadvantages. One advantage is that it eliminates the need for markers, which can be time-consuming and invasive (Lübbers et al. 2011). Markerless registration also allows for improved accuracy using a dynamic touchable region model (DTRM) (Nguyen et al. 2022). However, markerless registration can have limited accuracy due to the ambiguity of the correspondence point set (Lübbers et al. 2011).Furthermore, variability in the accuracy of implant position has been observed in fully edentulous patients, which can impact the accuracy of markerless registration (Ekram et al. 2022, Lübbers et al. 2011). Thiem et al. conducted a comparative analysis between marker-based and marker-free methods for navigation-assisted surgery and observed that in edentulous patients marker-free methods generally exhibit lower levels of accuracy and reproducibility (Thiem et al. 2022). Nonetheless, Ekram et al. conducted a retrospective study comparing various registration techniques in fully edentulous patients and concluded that there is no significant difference in accuracy between marker-free approaches, gutta-percha markers, and barium sulphate scan appliance methods (Ekram et al. 2022). Furthermore, a study proposed a surface-matching method using a portable 3D scanner for patient-to-image registration in neurosurgery, which demonstrated sufficient accuracy even in the posterior area of the head (Fan et al. 2014).
What are the challenges in markerless registration for fully edentulous patients?
The process of markerless registration for fully edentulous patients presents several distinct challenges. One of the primary obstacles is the deformation of the facial structure during surgery, as the face does not exhibit uniform deformability. This deformation can have an adverse impact on the accuracy of markerless registration (Žgaljić et al. 2020).
Another challenge lies in the ambiguity associated with the correspondence point set, which inherently limits the precision of markerless registration. Addressing challenges in markerless registration for fully edentulous patients is crucial. A proposed registration framework utilizes a dynamic touchable region model (DTRM) to enhance registration accuracy (Nguyen et al. 2022, dos Santos et al. 2014). Markerless registration in fully edentulous patients requires capturing intraoperative patient anatomy using a range image device while addressing issues like severe non-rigid deformations and noise in acquired surface data (Žgaljić et al. 2020). Overcoming these challenges is essential for achieving accurate markerless registration in fully edentulous patients.
How can we improve the accuracy of markerless registration for fully edentulous patients?
To improve the precision of markerless registration in fully edentulous patients, it is advisable to consider the utilization of two digital data registration protocols. These protocols are designed with the goal of enhancing the precision of data acquisition and the superimposition of data onto planning software, ultimately leading to improved treatment outcomes. Additionally, dividing the facial surface into different regions and examining the deformability of each region can offer benefits in markerless registration. Through the utilization of regions that exhibit less deformability for registration purposes and the exclusion of highly deformable regions, the accuracy of markerless registration can be significantly enhanced. By incorporating these protocols, the accuracy of markerless registration can be improved, leading to more precise preoperative planning and implant placement (Nguyen et al. 2022, Žgaljić et al. 2020).
How does markerless registration compare to other registration methods for fully edentulous patients?
Markerless registration has been compared to other registration methods for fully edentulous patients. A study conducted by Ekram et al. revealed that the marker-free technique exhibited no significant difference in accuracy when compared to the barium sulphate scan appliance and gutta-percha marker methods (Ekram et al. 2022). A different investigation by Woo et al. discovered that the entire surface-based matching method, known as the markerless approach, exhibited greater precision in image registration for implant planning in fully edentulous jaws compared to the small point-based method (Woo et al. 2020). These findings indicate that markerless registration can be a viable option for fully edentulous patients, offering comparable accuracy to other registration methods.
Methods to reduce image artifacts from navigation markers in dynamic guided implant surgery
Different navigation markers could cause different degrees of artifacts, which would affect the accuracy and efficiency of the implant navigation system. Silicon nitride is the ideal material for registration in oral implant navigator-guided surgery owing to less artifact generation, better radiopacity and desirable abrasion resistance. Silicon nitride navigation markers have the best overall performance in registration. Aluminum oxide markers have the fewest artifacts, but silicon nitride is ideal (Du et al. 2019). Other possible solutions include use of complementary magnetic resonance images, augmented reality using dental cast model images obtained by CT, and metal artefact reduction (MAR) algorithms. More studies are needed to generate comprehensive solutions (Du et al. 2019).
What are the different types of registration errors?
There is a possibility of different types of errors occurring during registration, including fiducial localization error (FLE), which arises when locating the fiducial point; fiducial registration error (FRE), which involves errors in measuring the distance between corresponding fiducial points after registration; and target registration error (TRE), which represents errors in measuring the distance between corresponding points other than the fiducial point after registration. TRE is a commonly used index to evaluate registration errors as it represents the combined error after registering a specific surgical area. The number and distribution of registration markers have a significant impact on the accuracy of the registration process (Shen et al. 2019, Zhang et al. 2011).
Conclusions and recommendations
To conclude, the findings propose that these distinct techniques of registration have the potential to enhance the precision, efficiency, and safety of implant placement in patients who lack teeth. When selecting a registration method for fully edentulous patients, it is crucial to consider the clinical significance of accuracy and the specific area that requires coverage. Although invasive screw markers are frequently employed, they can result in additional trauma and discomfort for patients. As an alternative, non-invasive adhesive markers have been created and have demonstrated comparable accuracy to screw markers. For optimal registration accuracy, it is advisable to utilize a minimum of six registration markers in the upper jaw. The utilization of reflective wafers as a calibration method has been discovered to enhance efficiency and achieve comparable accuracy to other calibration methods. The implementation of intraoperative imaging, such as intraoperative CT scanning, permits automatic patient registration that is independent of user input, thus reducing the likelihood of registration errors. The utilization of low-dose protocols for initial registration scans using iCT scanning has been demonstrated to achieve minimal radiation exposure while maintaining navigation accuracy. The advent of novel 3D ultrasound acquisition allows for the referencing of anatomical structures within a broader field of view, making it a potentially valuable tool to supplement CBCT. It is imperative to conduct well-designed randomized control trials, and researchers should concentrate on developing a registration technique that overcomes the limitations of current methods while achieving clinically acceptable accuracy and reproducibility.
Would you like to read more about this topic?