Introduction
Precise recording of dental implant positions is critical for achieving an accurate and passive fit of full-arch, implant-supported fixed dental prostheses (iFDP) (Rutkūnas et al., 2017; Pozzi et al., 2022; Pradies et al., 2013). Intra-oral optical scanning (IOS) has been extensively utilized to obtain digital impressions for single-unit or short span multi-unit iFDPs (Wang et al., 2024). For full-arch iFDPs, IOS also reported clinically acceptable results as compared to conventional impressions in systematic reviews (Pesce et al., 2024; Pesce et al., 2018). However, the size of the edentulous span negatively affects the accuracy of IOS, as the lack of natural reference objects can cause splicing errors and overlaps, leading to errors or the inability to recognize the data (Gómez-Polo et al., 2022). Moreover, most of the studies in these reviews were based on in-vitro models and lacked consistency. Various adjunctive techniques – such as splinted scan bodies, snap-on or extended horizontal scan bodies, and auxiliary devices (scan ladder, fiducial markers) – have also been proposed to enhance IOS accuracy in full-arch implant impressions (Shetty et al., 2025; Aruri et al., 2025, Nulty., 2024). As digital implant dentistry continues to evolve, extra-oral photogrammetry offers an alternative approach to enhance precision of full arch-implant impressions (Negreiros et al., 2025).
Photogrammetry employs a sequence of high-resolution images obtained from multiple angles to estimate the 3D spatial locations of implants. Extra-oral photogrammetry (EPG) uses a multi-lens camera and specialized scan bodies to triangulate precise implant locations in dentistry without the need for stitching techniques or soft tissue landmarks (Agustin-Panadero et al., 2015; Altalla et al., 2025). A systematic review assessed the accuracy of IOS and photogrammetry in capturing full-arch implant impressions and concluded that photogrammetry is a more reliable technology than IOS to capture implant positions for full-arch rehabilitations, exhibiting significantly greater trueness and precision (Pozzi et al., 2025). It is important to note that EPG only captures the three-dimensional positions of implants and does not record the surrounding soft tissue morphology. Therefore, an additional IOS remains necessary to capture soft tissue contours and gingival architecture for a complete and accurate digital prosthesis design (Negreiros et al., 2025).
The Significance of EPG in Full-Arch Cases:
Exquisite accuracy and passive fit are of high relevance for multi-unit iFDPs. Conventional techniques, such as intraoral scanning or open-tray impressions, may generate mistakes because of things like:
- Implant angulation
- Soft tissue distortion
- Scanner stitching inconsistencies
- Patient movement
On the other hand, photogrammetry systems (such the iCAM4D and PIC systems) provide:
- Ultra-high accuracy and consistency
- Verification jigs and splinting are not necessary
- Decreased patient discomfort and chair time
Clinical Workflow:
1. EPG scan:
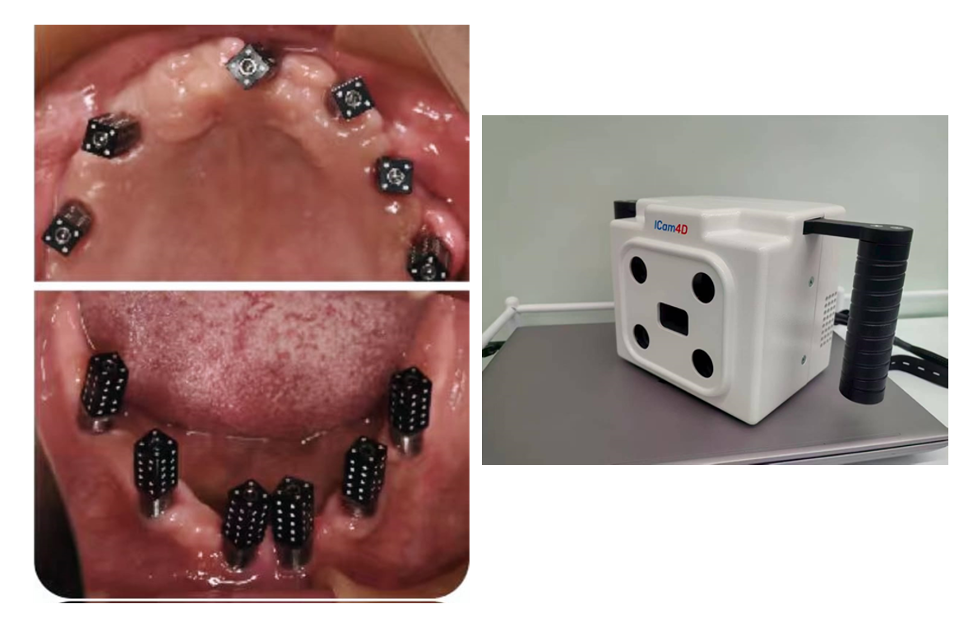
Compatible photogrammetry scan bodies (ICAM scan bodies) are placed on all implants and hand-tightened. The scan bodies have a coded geometry which is identified by the camera system. The EPG device is calibrated using the calibration device and following the protocol endorsed by the manufacturer (Fig. 1).

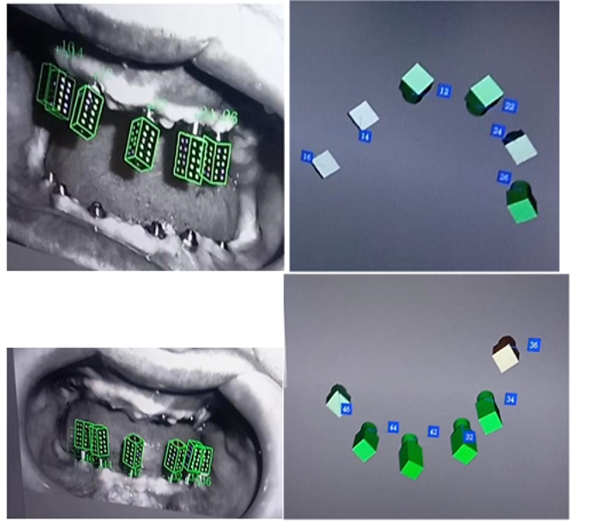
The photogrammetry camera (ICAM4D or PIC) is set up to capture multiple pictures from various angles around the arch with a scanning distance ranging from 25 to 30 cm. This step registers the exact 3D coordinates and precise angulations of all implants simultaneously. After the acquisition of PG scan, the STL file is generated that represents the implant positions (Fig. 2)
2. Intra-oral scan
Scan bodies are inserted and hand-tightened to obtain a digital impression. A digital intra-oral scan is performed to record the soft tissues and mucosal contours.
3. Integration of IOS & EPG scan
First, the scan bodies of IOS are aligned with the standard scan bodies in the database. Then, the aligned standard scan bodies are matched with the extra-oral scan bodies of the EPG scan (Fig. 3)
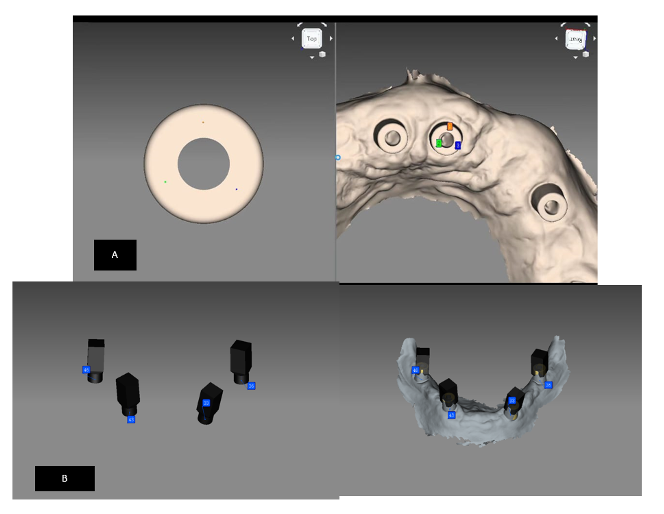
Figure 3: Integration of intra-oral scan with scan bodies of database (A); and aligning of scan bodies with the scan bodies of EPG (B); complete integration (C)
4. CAD /CAM Design:
Based on the aligned digital data model, with the EPG scan containing the implant locations and the IOS file containing the soft tissue contours, the iFDP is digitally designed (Figs 4 & 5)
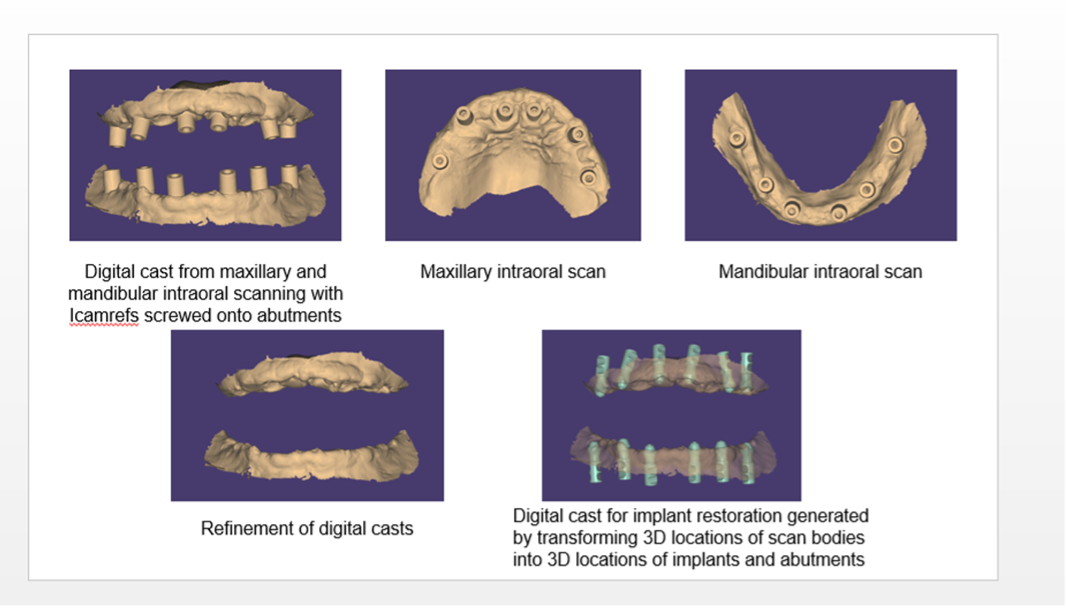
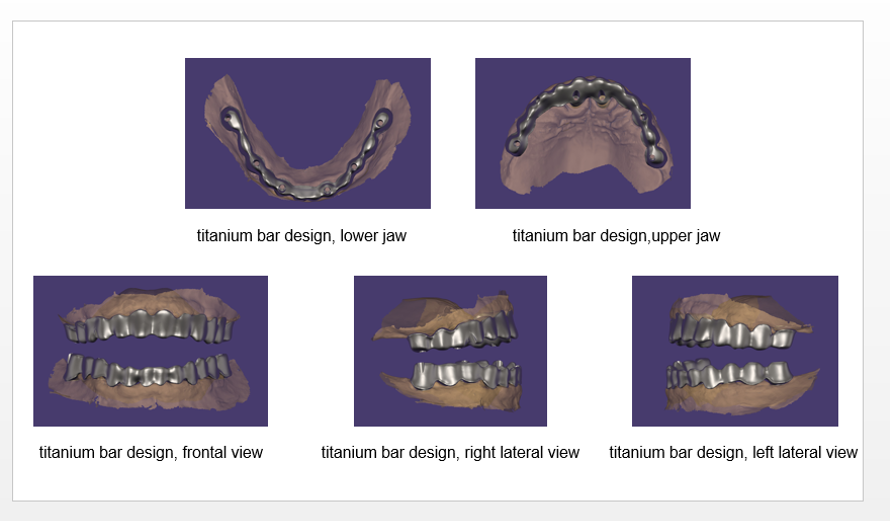
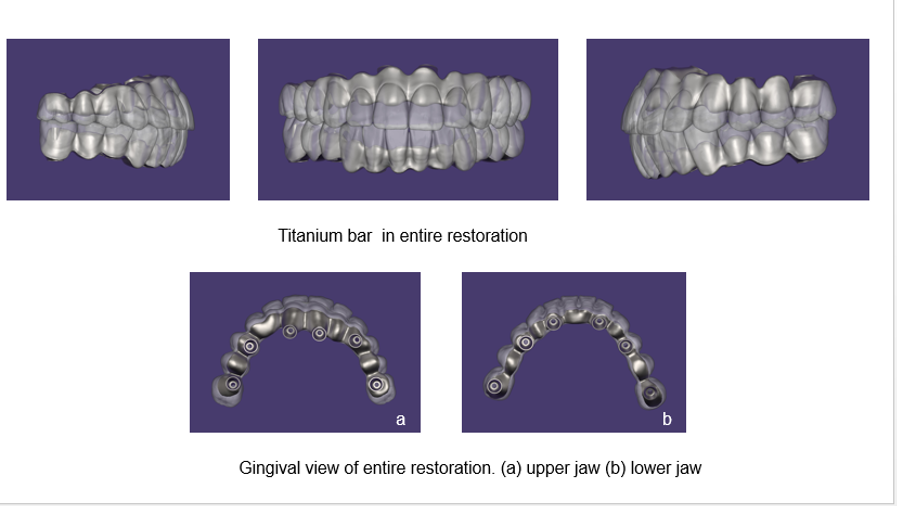
Figure 5: Designing titanium bar for the definitive iFDP
5. Fabrication and Delivery:
The designed prosthesis is fabricated by means of milling or 3D printing. After a try-in and clinically verified fit, the iFDP can be delivered.
Advantages of Photogrammetry:
- High accuracy specifically in full arches
- Passive fit of frameworks
- Digital integration with CAD/CAM
Limitations:
- Intra-oral scan is needed for soft tissue digitization
- Higher cost of the equipment
- Training required for use
- Dependent on scan body precision and correct camera positioning
Summary:
As mentioned above, the EPG is only capable of recording implant positions; therefore, an additional IOS is needed to capture the soft tissue morphology. To overcome this limitation a new intra-oral device was developed that integrates the intra-oral scan and intra-oral photogrammetry (IPG) (Pozzi & Laureti et al., 2025). This device automatically generates a single STL file that includes implant positions, jaw anatomy and occlusion in one scan. For this process, two different scans are obtained: one to capture the implant positions by intra-oral photogrammetry and the second to capture the soft tissue anatomy by an intra-oral scan. A different set of scan bodies has to be used for these two scans.
However, in contrast to EPG, only one device is needed to capture both scans, and the scan files are automatically aligned. Hence by combining the accuracy of photogrammetry with IOS ability to capture soft tissues, this system may offer a more efficient and practical approach to complete arch implant-retained impressions (Negreiros et al., 2025). However, the evidence on IPG and its trueness and precision for full-arch iFDP is still limited.







