
Angulated Screw Channel Solutions
The provision of an implant-supported restoration presents many challenges for the dental clinician, especially in the atrophic maxilla. This is due to a myriad of factors like atrophy of the residual ridge, facial morphology, inclination of the implant axis and other factors (Mericske-Stern et al. 2000). The fabrication of an implant restoration in such a case would usually require use of additional components to provide an angulation change or to use a cement-retained restoration if the access channel is too buccally or lingually placed (Berroeta et al. 2015). Wherever feasible, screw-retained restorations are preferred over cement retention due to disadvantages such as the difficulty of cleaning excess cement and decreased retrievability (Agar et al. 1997). If there is residual cement around implant restorations, it was found to be associated with clinical and radiographic signs of peri-implant disease (Wilson Jr. 2009). On the other hand, if additional prosthetic components are used to change the angulation yet still maintaining the screw-retained design, it will incur additional costs and introduce more complexity at the implant-prosthetic connection.
The recent development of an angulated screw channel abutment provided an alternative way of maintaining a screw-retained prosthetic restoration under such circumstances. Through a screw-retained implant restoration, we can achieve more predictable retention and retrievability, and avoid the biological consequence of residual cement with a cemented retained implant restoration (Priest 2017).
A study by Friberg and Ahmadzai (Friberg and Ahmadzai 2019) on the restoration of parallel-walled implants with conical connections showed that implant survival rate could be as high as 98%, and a restoration survival rate of 100% after one year of function when an angulated screw channel system is used. There was limited peri-implant bone loss noted in both the study by Pol et al. (Pol et al. 2020) at 0.16mm, and 0.41mm peri-implant bone loss in the study by Friberg and Ahmadzai. These results are similar to those of other studies on identical implant designs without the use of angulated screw channels.
A survey done by Pol et al. also looked at patients’ satisfaction with implants restored with angulated screw channels in terms of esthetics, function, and overall satisfaction. Their survey found that the overall satisfaction with implants restored with angulated screw channel solutions was comparable to those of other studies. Additionally, angulated screw channel systems have not been found to increase technical complications (Anitua et al. 2020) and esthetics and functional results are comparable to those with cement-retained crowns (Nastri et al. 2021).
How it works
The angulated screw channel concept consists of two main features (Mulla et al. 2021):
- Screw head with hexalobular design
- Special screwdriver that can engage the screw at any angle between 0 to 28 degrees with 360 degrees with rotational freedom
An illustration of an angulated screw channel abutment is shown in Fig. 1 (Nastri et al. 2021):
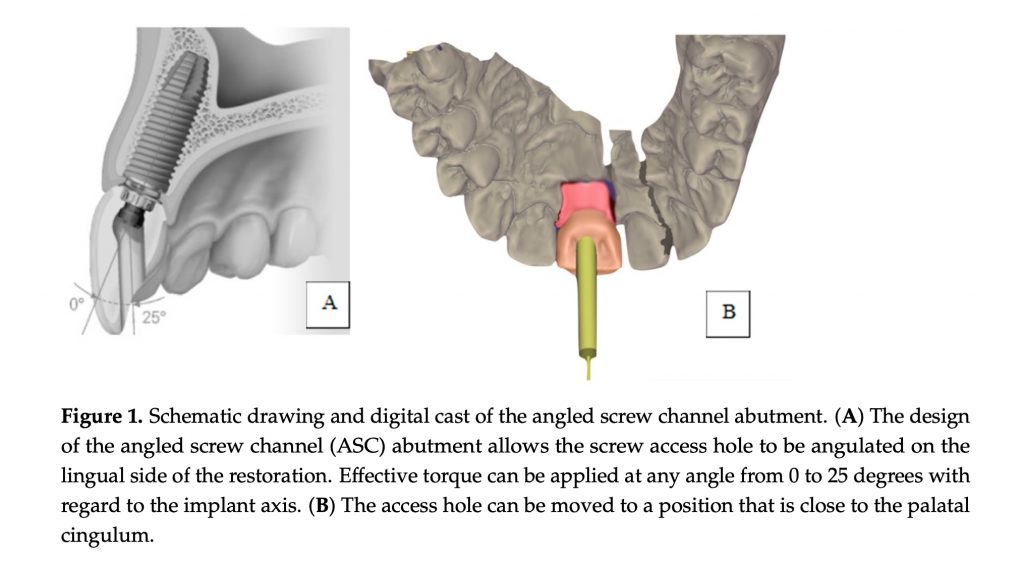
The angulated screw channel system can come either as a castable abutment or a Ti-base. A castable abutment comprises two pieces connected by an elbow that works as a joint, while the chimney pivots on the semi-spherical base. The fixation screw is unique and allows tightening with a screwdriver while off-axis (Berroeta et al. 2015). For an angulated screw channel Ti-base, the screw head can sit on a pre-fabricated Ti-base with the final prosthetic restoration cemented onto the Ti-base. Some systems consist of a Ti-base where the prosthetic restoration will be friction-fitted onto the Ti-base, with the screw head sitting on the internal surface of the restoration. The screwdriver can usually engage the screw head at any degree up to 30 degrees. The final torque of the screw is usually 20-35Ncm.
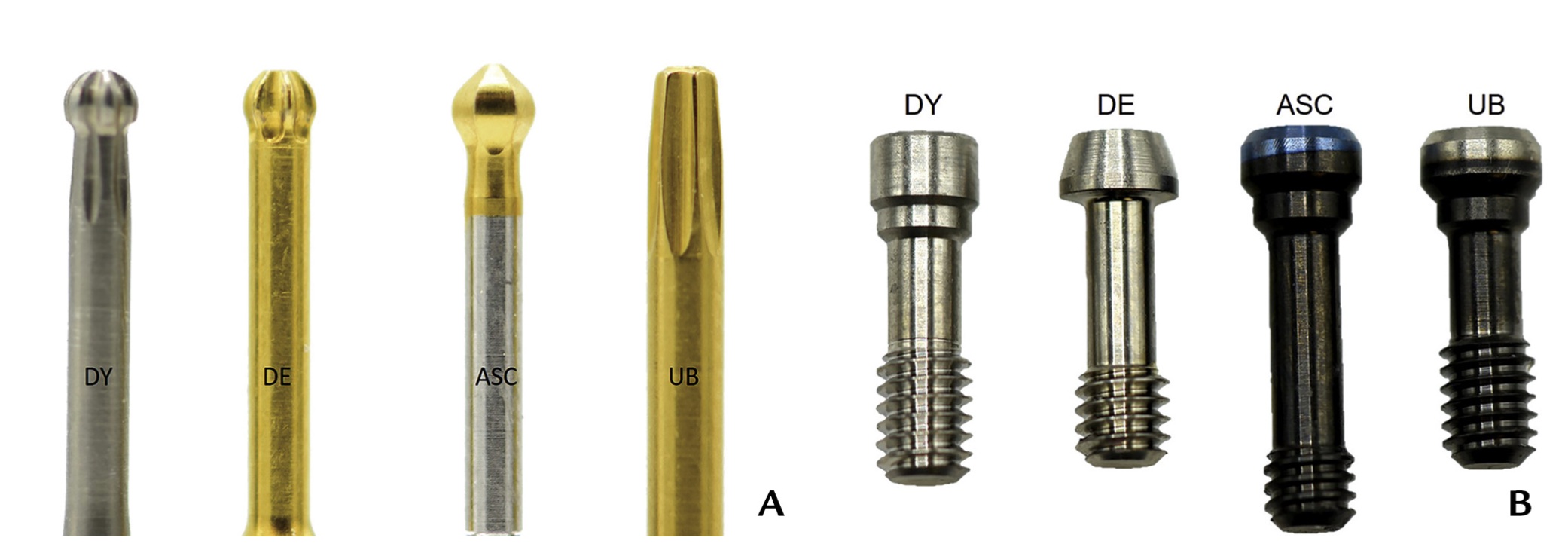
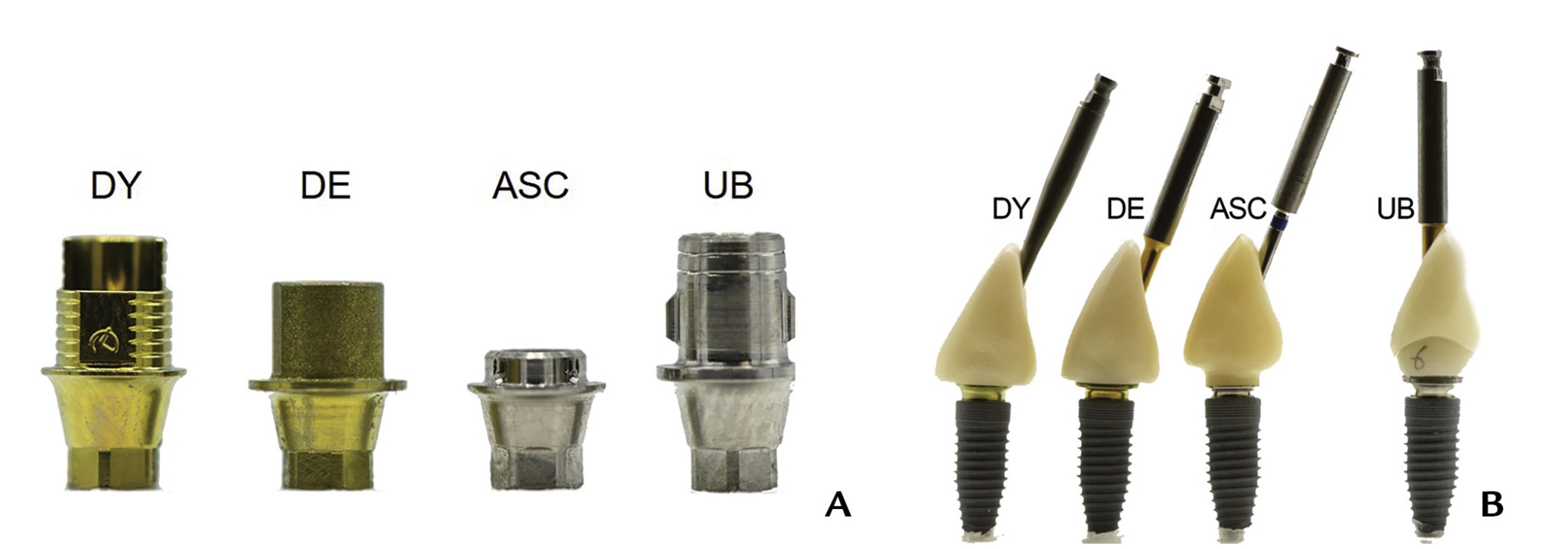
Some examples of hexalobular screwdrivers and the corresponding abutment screws are shown in Fig. 2 & Fig. 3 (Mulla et al. 2021):
An example of the hexalobular screwdriver and corresponding abutment screws for the Straumann Angled Solution System as shown in Figs 4-7:



Indications and contraindications for usage
Indications:
- Off-axis inclination up to indicated degrees of change by the manufacturer (25-30 degrees)
- Appropriate treatment planning
- Good lab support
Contraindications:
- Off-axis correction greater than manufacturer’s instructions
- Inadequate lab support
The angulated screw channel system should not be considered a one-fits-all solution for any implants placed in a non-ideal implant position. There is a limitation to the angle of degree change, and its usage should be considered as an alternative when presented with unfavorable circumstances for placing an implant in an ideal position.
Appropriate treatment planning and restoration-driven implant planning should be carried out before insertion of the implants to assess and plan for the degree of angulation change whenever possible. In some cases, the design of the abutment to allow for alteration in the engagement of the screw could result in inadequate thickness of material at the junction where the screwdriver engages the screw. The thickness of the prosthetic material may have to be increased to prevent the material from fracturing, which may affect the emergence profile as well as the esthetics of the prosthesis.
Extra consideration should also be given to the esthetic concerns in the anterior region. The use of angulated screw channel systems may sometimes be unable to compensate for any esthetic compromise with the placement of an implant in a patient with a high smile line. If the implant is placed too far facially and of an inadequate depth/shallow facially, there may be show-through of the abutment junction as a grayish shadow through the buccal mucosa that may not be able to be corrected. As such, implants should ideally be planned to be placed at a depth of 3mm below the cemento-enamel junction to allow for optimal planning of the emergency profile and esthetics of the restoration (Jivraj and Chee 2006).
The height of the Ti-base abutments on some systems is an additional factor to be considered. A shorter abutment height that allows for rotational freedom could also result in less area for engagement of the abutment with the dental prosthesis, leading to decementation of the prosthesis from the abutments under functional loading.
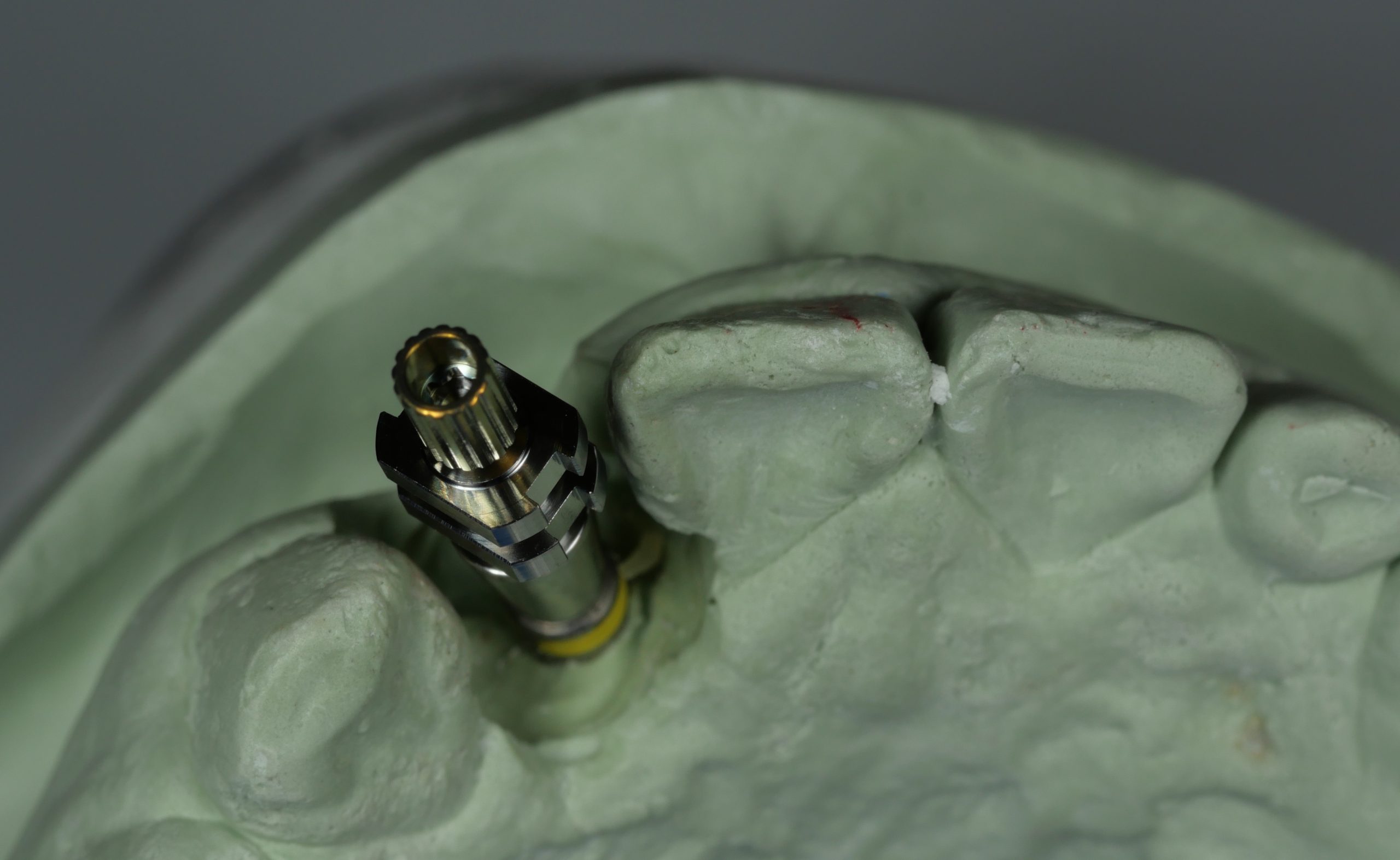
Clinical case examples
Case 1



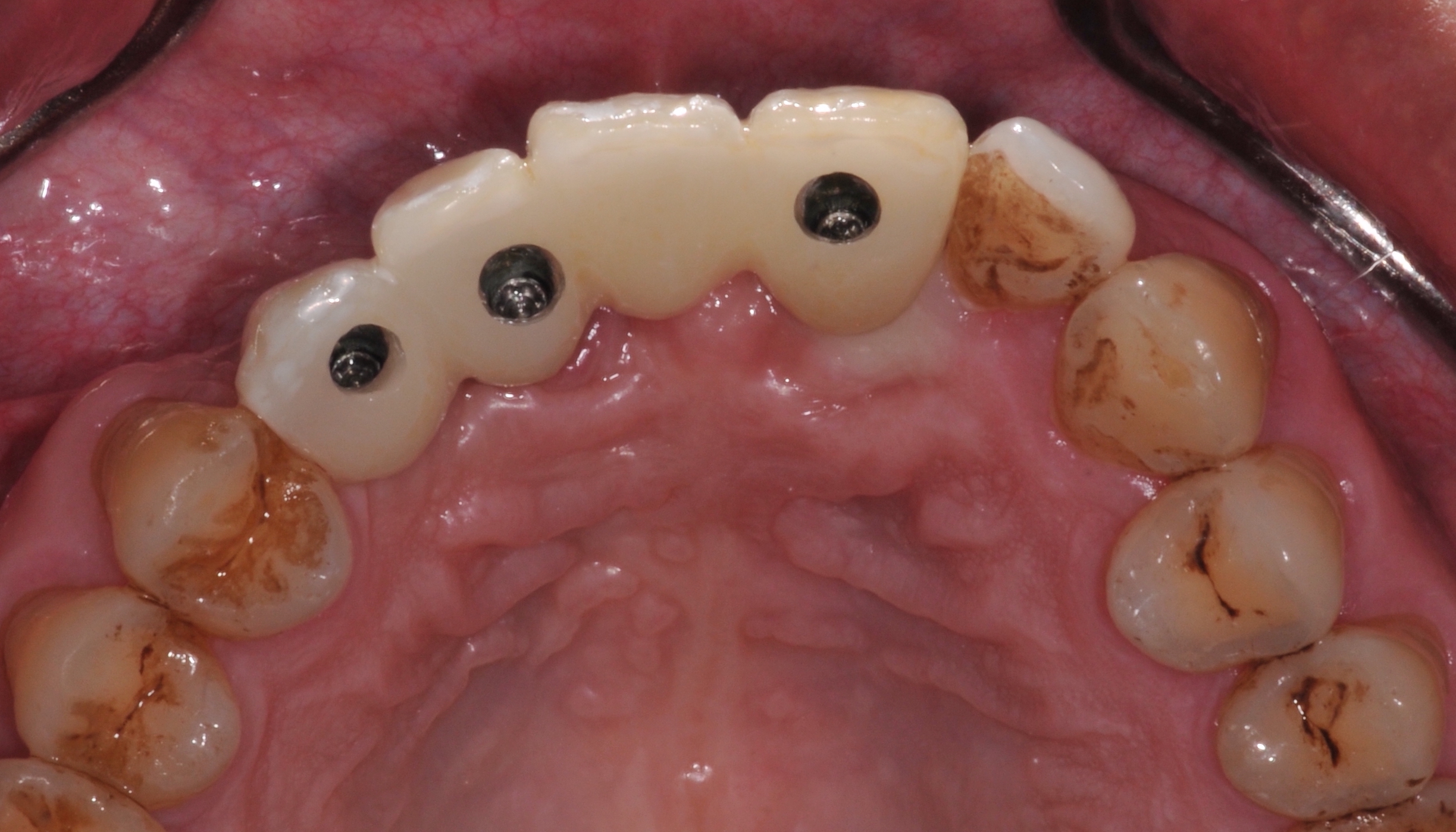
Case 2



Conclusion
The hexalobular screw design of the angulated screw channel solution allows the torque to be applied to the screw on a nonaxial axis. There has been some research into applying torque in a nonaxial direction and how the reverse torque values (RTVs) are affected by cyclic loading compared with systems where the torque is applied in a straight screw axis. A study by Goldberg et al. (Goldberg et al. 2019) found that angulation had no effect on RTVs. Some studies on samples with no cyclic loading showed significantly reduced RTVs with increased angulation change. There was some speculation that at higher degrees of angulation change, the asymmetry of the hexalobular driver head may result in inadequate engagement of the abutment screw to apply the relevant torque (Hu et al. 2019).
However, Mulla et al. then conducted a study to examine the effect of cyclic loading on the RTVs. The RTVs of 25-degree angulated screw channel systems with hexalobular designs were compared to crowns cemented on 0-degree screw channel abutments after cyclic loading. Their study found that angulated screw channel solution systems with higher initial recommended torque values (35 Ncm) may show a similar performance to that of conventional straight-access abutments in term of RTVs. Swamidass et al. found similar results where they looked at the percentage torque loss. As such, angulated screw channel systems should be expected to have comparable maintenance of the screw torque as conventional screw channel abutments.
Different angulated screw channel systems are available from implant manufacturers and independent manufacturers. While in the study by Frieberg and Ahmadzai, there was no notable improvement in esthetics with the use of original components, they did report an observation by clinicians of a larger palatal access hole with non-original components. Some systems such as the Straumann Angled Solutions (Straumann AG, Basel, Switzeland) have also been stated to have the advantage of a reduced screw access channel diameter that reduces the risk of chipping.
As such, in selecting an angulated screw channel system, it may be worth considering the use of an angulated screw access channel system with a higher recommended initial torque value (e.g 35Ncm) and with a reduced screw access channel diameter where possible.
It is also important to note the right case selection and consider the indications and contraindications in using of such abutment systems. Lastly, communication with the laboratory on their ability to support the fabrication of prostheses compatible with angulated screw channel components is critical to the successful fabrication of final restoration.





