
Abstract
The case report describes how the implant process can be streamlined by combining a surgical guide with a temporary restoration. A 54-year-old male patient presenting with partial edentulism underwent computer-aided, template-guided implant placement to replace the missing tooth 12 (FDI-system). Implant bed preparation was then performed using the bridge as a surgical guide. After osteotomy, the guidance sleeve within the bridge was sealed, and the bridge was temporarily incorporated for submerged healing of the implant. The usage of a temporary restoration as a surgical guide seems to make the digital workflow of guided implant placement more efficient by achieving a predictable clinical outcome.
Background
Nowadays, dentistry is not just about dealing with pain and restoring function. Today’s patients are well informed and not always satisfied by simple prosthetics (Siddique et al., 2019). This results in an increased demand for predictable, esthetic treatment solutions, especially in the anterior region (Korfage et al., 2018). For high-level esthetic outcomes, the three-dimensional implant position in the edentulous site has to be chosen carefully (Su et al., 2014), whereby the implant is thought of as an apical extension of the ideal future restoration. This fact is the key principle of backward planning (Schubert et al., 2019).
After preoperative planning, the defined implant position has to be transferred to the clinical site. In the literature, methods for that transfer are divided into two main categories: free-hand and guided (Nickenig et al., 2010). With the advancement of prototyping technologies, surgical guides can now be created more rapidly and with greater precision. This development also opens new possibilities for innovative approaches to guide design (Neugebauer et al., 2010). In terms of accuracy, the superiority of surgical guides over the free-hand method has been clearly demonstrated (Nickenig et al., 2010; Alevizakos et al.; Arisan et al., 2013; Vermeulen, 2017).
After successful implant placement, a temporary restoration is needed, especially in the anterior region, which has higher esthetic demands (Turkyilmaz et al., 2009). As implant healing can last up to 6 months, the clinician has the opportunity to test the shape and color of the final restoration, and correct it, if necessary, by modifying the temporary restoration (Al-Harbi & Edgin, 2007; Di et al., 2012; Norton, 2004). Nowadays, temporary restorations in implant dentistry can be manufactured by computer-aided design and computer-aided manufacturing (CAD/CAM) systems (Abdullah et al., 2016). With these systems, the production of the temporary restoration is more predictable, and the materials used are more resistant to abrasion and staining than conventional temporary restorations (Norton, 2004; Abdullah et al., 2016).
This case report describes guided implant placement in the anterior region using a temporary bridge as a surgical guide. The rationale for utilizing a temporary bridge as a surgical guide is based on the need to ensure optimal implant positioning in the esthetic zone, where accuracy is critical to both functional and esthetic outcomes. This method allows for better intraoperative visualization and enhanced control over implant placement, ultimately contributing to improved patient satisfaction and clinical results.
Case presentation
The patient’s consent was obtained for the publication of this case report. A 54-year-old male patient presented with an esthetically and clinically insufficient fixed partial denture (FPD) with abutment teeth 11 and 13 for the replacement of a missing tooth 12 (Fig. 1). The patient demanded an implant solution.

Fig. 1: The esthetically and clinically insufficient dental bridge (11–13)
The treatment plan was to replace the dental bridge with two full-ceramic crowns on teeth 11 and 13 and an implant-supported full-ceramic crown in region 12. During the implant healing process, the edentulous region 12 would be restored using a temporary bridge.
Since the treatment involved the esthetic region, and in accordance with the SAC Assessment Tool (ITI, Basel, Switzerland), a decision was made to proceed with implant placement only after thorough preoperative planning following the principles of backward planning and utilizing a surgical guide. To optimize the treatment protocol, we combined the surgical guide with the temporary bridge, resulting in an FPD-shaped guide.
Guide design and manufacturing
After removing the inadequate FPD, the preparation line of the abutment teeth was redefined, and the abutment teeth were scanned (Omnicam, Dentsply Sirona Deutschland GmbH, Bensheim, Germany). Using CAD/CAM software (Cerec 4.4.2, Dentsply Sirona Deutschland GmbH, Bensheim, Germany), a dental bridge was designed as a virtual wax-up on the scanned abutment teeth (Fig. 2). The bridge was exported as an STL file and imported together with the cone-beam computer tomography (CBCT) scan into the planning software (coDiagnostiX, Straumann, Basel, Switzerland). During planning, the bridge was matched with the teeth as prepared on the CBCT scan (Fig. 3). Using the principles of backward planning, the implant position was adjusted as necessary (Fig. 4). Subtracting the implant axis, visualized as a bar from the FPD, a slot was implemented into the bridge (Fig. 5). The restoration was exported and sent for milling (inLab MC X5, Dentsply Sirona Deutschland GmbH, Bensheim, Germany). Two bridges were manufactured (inLab MC X5, Dentsply Sirona Deutschland GmbH, Bensheim, Germany): a zirconia FPD for the surgery and a polymethylmethacrylate (PMMA) FPD (IPS e.max ZirCAD and Telio CAD, Ivoclar Vivadent AG, Schaan, Liechtenstein). Both FPDs were post-processed according to the manufacturer’s instructions (Fig. 6). The reason for fabricating two bridges lies in the specific requirements of the treatment. The zirconia FPD was designed for use during surgery and throughout the healing period, chosen for its high strength and fracture resistance, which ensures durability during and after the implant placement procedure. Conversely, the PMMA FPD was made as a provisional bridge to protect the abutment teeth until surgery took place. PMMA is a cost-effective material with excellent biocompatibility, making it suitable for short-term use while providing necessary protection prior to surgery. This combination ensures both efficient temporary protection and long-term stability post-surgery.
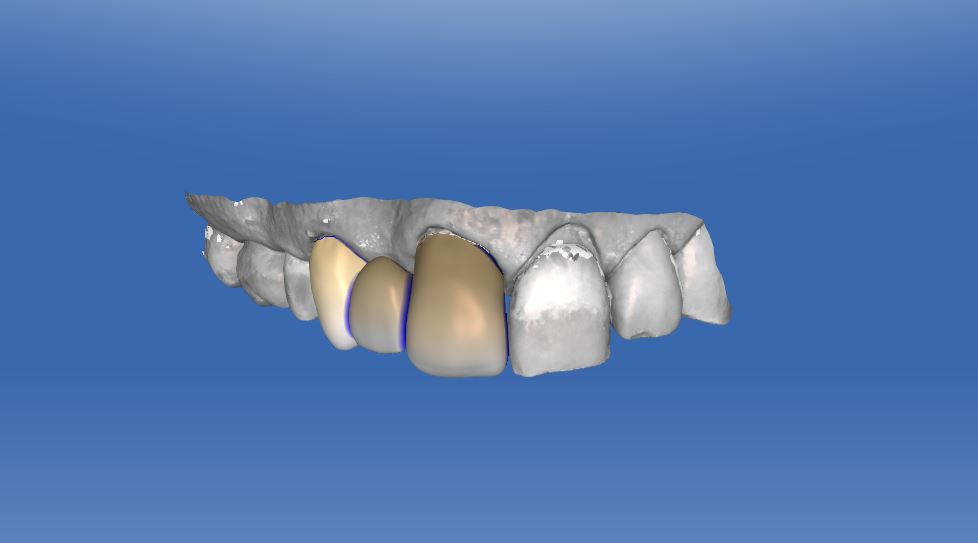
Fig. 2: CAD-designed dental bridge (11–13) 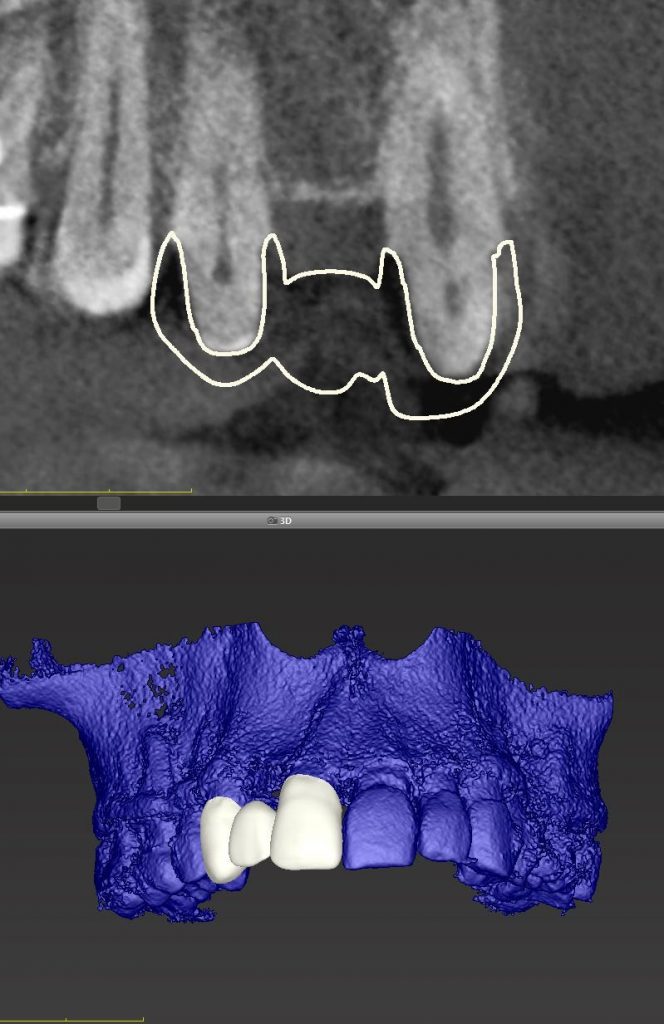
Fig. 3: Bridge imported into the planning software 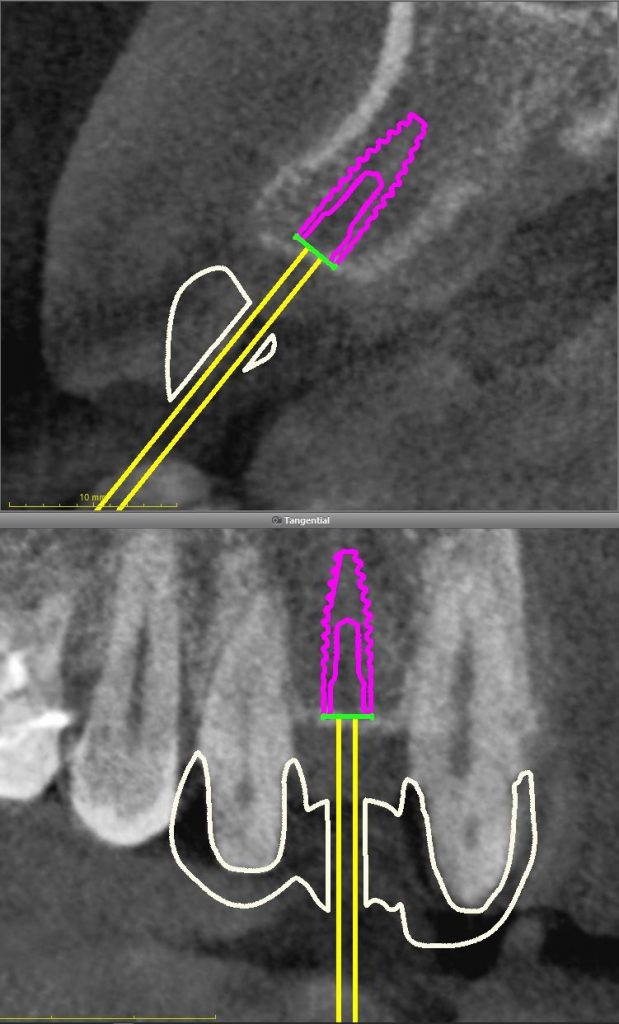
Fig. 4: Prosthetically driven implant positioning 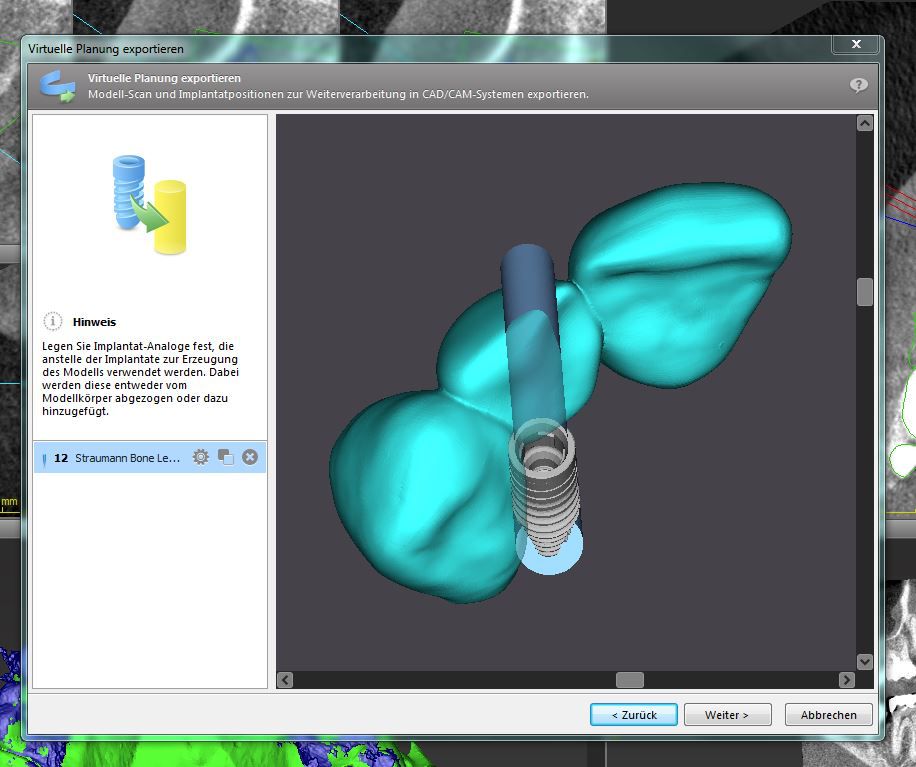
Fig. 5a: Implementing a slot into the bridge – surgical guide 
Fig. 5b: Implementing a slot into the bridge – surgical guide 
Fig. 6: The post-processed zirconia FPD
Guided surgery
The temporary cemented PMMA FPD was removed, the abutment teeth cleaned, and the guide was placed on the prepared teeth to mark the field of interest (FOI). After raising the flap to facilitate submerged healing, drilling was performed using the surgical guide (Fig. 7). The opening for the drill was designed based on the manufacturer’s specifications to accommodate the initial drill, which has a diameter of 2.24 mm. The fit is intentionally snug to ensure precision during the drilling process, minimizing lateral movement. To reduce the risk of debris coming into contact with the bur, we ensured that drilling was performed with constant irrigation. A diameter-reduced implant (D 2.9 mm L 10 mm, Bone Level Roxolid SLAtive, Straumann, Basel, Switzerland) was inserted, achieving a primary stability of 30 Ncm (Fig. 8). A control X-ray was made showing the correct implant position with sufficient distance from the adjacent teeth (Fig. 9). The field of intervention was covered with soft tissue and sealed with one suture. The drilling hole in the bridge was sealed with composite, and the bridge was fixed on the teeth using temporary cement. The sutures were removed seven days after the operation. Six months after implant placement, the temporary bridge was removed and replaced by the three individual crowns (Fig. 10).

Fig. 7: Osteotomy using a Provisional Restoration as a Guide 
Fig. 8: Implant placement 
Fig. 9: Post-operative X-ray 
Fig. 10: Post-op photo of the patient from the facial, with three individual crowns in place
Discussion
Modern CAD software makes it possible to plan and fabricate prosthetic restoration using virtual implant positioning, leading to more predictability in esthetic results.
This clinical case report demonstrated a different approach to production management in the digital workflow of implant placement. In the literature, several studies have discussed the surgical template as a general surgical guide (Alevizakos et al.; Arisan et al., 2010; Behneke et al., 2012; Bover-Ramos et al., 2018; Eggers et al., 2009; Horwitz et al., 2009; Lal et al., 2006). Within the present case report, a composite of the surgical guide and temporary restoration replaced the typical surgical template. As was shown in the postoperative X-ray, no adjacent teeth or sensitive anatomic structures were injured after implant placement, and the placement of the implant was prosthetically driven. Comparing the workflow presented with the usual method of guided implant placement, the surgical-template-fabrication phase was skipped, thus increasing workflow efficiency.
Regardless of the surgical guide used in surgery, precise matching of the intraoral scan (STL file) and the segmentation model of the three-dimensional X-ray (DICOM file) is mandatory for guide fitting and later implant positioning (Arisan et al., 2013; Mangano et al., 2018; Vercruyssen et al., 2014). For precise superimposition, common landmarks, both on the 3D dataset of the intraoral scan as well as the segmentation model of the preoperative CBCT, were manually selected.
Incorrect superimposition of the CBCT and intraoral scan and insufficient fixation of the surgical guide during implant surgery might result in a poor esthetic outcome and violation of adjacent anatomical structures due to incorrect implant placement (Lee et al., 2013; Schnutenhaus et al., 2018; Jones, 2018; Seo & Juodzbalys, 2018; Hanif et al., 2017).
The guide should be supported by the least number of teeth as is reasonably achievable to minimize the influence of mismatch between the CBCT and intraoral scan on the implant position. This technique reduces the risk of mispositioning of the surgical guide as it can be fixed to the adjacent teeth.
From the literature, it is known that surgical guides decrease the amount of irrigation solution reaching the drill (Liu et al., 2018). The sleeve-holding part of the common guide in particular works like an umbrella that deflects irrigation from the drill (Liu et al., 2018). For traditional guides, different approaches have been presented in order to overcome the heat issue (Alevizakos et al., 2020). One of them is to design internal irrigation channels within the guide, allowing the irrigation solution to reach the drill through the guide (Alevizakos et al., 2020). In terms of irrigation, the FPD-shaped guide seems to block irrigation less than conventionally shaped guides.
In the future, it might be conceivable that a definitive FPD be used as a guide in similar cases and that after implant placement, this FPD be processed to single crowns. From a financial point of view, combining the prosthetic restoration with the surgical guide not only saves time but also saves on the cost of fabricating a guide. To achieve greater cost efficiency, modern CAD/CAM provisional materials (e.g., PEEK) could be used instead of zirconia for the temporary restoration or surgical guide. This approach involves planning, fabrication, and post-processing being completed in a single streamlined process. Additionally, the patient would require fewer appointments, positively impacting overall treatment efficiency. These assumptions should be further investigated to validate their effectiveness.
Conclusion
The usage of a temporary bridge restoration as a surgical guide might make the digital workflow of guided implant placement more efficient and increase the accuracy of implant placement. Furthermore, the workflow presented can also be transferred to other clinical cases, for instance, dentures. However, further studies are needed to confirm the possible advantages of the efficiency of this method.
Clinical relevance
The bridge-shaped guide might allow for higher efficiency in daily practice along with the other advantages of the conventional surgical guide.




