
Introduction
Rehabilitation with implant-supported fixed complete dental prosthesis (IFCDPs) requires a high level of congruence between the three-dimensional implant positions and the definitive prosthetic framework to ensure predictable long-term clinical outcomes. A passive fit, defined as the absence of strain at the implant-prosthesis interface, remains a fundamental principle to minimize mechanical complications, such as screw loosening or framework fracture, as well as biological complications including peri-implant bone loss (Arcuri et al., 2019; Goodacre et al., 2003). Although numerous investigations have attempted to define and quantify the acceptable degree of misfit, no universal consensus has yet been established (Abduo et al., 2010; Kan et al., 1999). Several authors have suggested that a marginal discrepancy of up to 150 µm may be clinically acceptable without compromising outcomes (Brånemark, 1983; Jemt, 1991; Klineberg & Murray, 1985). The accuracy of transferring implant positions is characterized by two primary metrics: trueness and precision, as outlined in ISO 5725–1 (International Organization for Standardization [ISO], 1994). Trueness refers to the closeness of a measurement to the actual value, while precision indicates the consistency of repeated measurements (Flügge et al., 2016; Pozzi et al., 2025a). Consequently, accurately transferring the implant location from the oral environment to the master model is a critical step in achieving a passive fit of the final prosthesis.
Conventional Full-Arch Implant Impression
Traditionally, the open-tray, splinted coping impression technique has been regarded as the gold standard for full-arch implant prostheses (Papaspyridakos et al., 2014; Pozzi et al., 2013; Moreira et al., 2015). However, this conventional workflow involves multiple steps in the production of a master cast, each of which introduces potential errors. These include the impression procedure, transport to the laboratory, and cast pouring steps that are inherently influenced by the physical properties and limitations of dental materials (Del’Acqua et al., 2008). Additionally, the procedure is time-consuming and can be uncomfortable for patients (Goodacre et al., 2003). Digital workflows have streamlined dental impression procedures through the introduction of intraoral scanning, replacing traditional analog materials to mitigate the inherent limitations of conventional analog techniques.
Digital Full-Arch Impression
Intraoral Scanning (IOS)
There are five primary complete-arch implant scanning techniques performed with IOS: non-splinting, non-calibrated splinting, calibrated scan bodies, calibrated frameworks, and reverse-impression methods (Revilla-León et al., 2025c). As each technique follows a different digital workflow, understanding their distinctions helps clinicians select the most appropriate method for accurate digital implant capture. IOS accuracy can be influenced by operator-related factors such as scanner type, head size, calibration, scanning distance, environmental conditions, and scanning strategy, as well as patient-related factors including tooth morphology, interdental spacing, arch form, soft-tissue conditions, existing restorations, edentulous regions, implant configuration, and scan body selection (Rutkunas et al., 2023).
Although IOS has been widely adopted for single or short-span implant restorations, its accuracy in full-arch implant prostheses remains a subject of debate, particularly in the mandibular arch (Abduo et al., 2010; Nedelcu et al., 2023). The main limitation of IOS lies in its three-dimensional (3D) image reconstruction, which depends on best-fit algorithms that stitch overlapping images by identifying common reference points. Each stitching step introduces minor deviations, which accumulate over longer edentulous spans with limited stable anatomical landmarks (Flügge et al., 2016). While artificial markers have been proposed to optimize scanning accuracy, these methods are not completely error-free and can present practical challenges in clinical application (Papaspyridakos et al., 2014; Rivara et al., 2016).
Horizontally oriented SBs and grammetry systems have recently been introduced to enhance implant scanning accuracy. Unlike conventional vertical SBs, horizontally oriented SBs in various dimensions enhance accuracy by reducing inter-SB gaps and inconsistencies. This configuration enables a smoother single-pass scanning workflow and minimizes overlap-related stitching errors along the arch, consistent with principles observed in splinted SB techniques (Azevedo et al., 2025). Conversely, grammetry uses splinted scan bodies such as OptiSplint to achieve micron-level accuracy with a standard intraoral scanner for generating the digital impression. These splinted scan bodies can also be used to verify a physical cast, thereby integrating both digital and analog workflows. However, one study reported that although grammetry improved the trueness of complete-arch implant scans, it did not confer a corresponding positive effect on their precision (Prott et al., 2025).
Photogrammetry (PG)
Photogrammetry has been introduced to mitigate inherent IOS stitching errors as it does not rely on intraoral anatomical landmarks. This method reconstructs spatial positions from multiple overlapping photographs, which are then processed by specialized software to generate a 3D model of the implant positions. In dental implantology, three main PG systems are employed (Fig. 1): extraoral photogrammetry (EPG), intraoral photogrammetry (IPG), and navigation-assisted photogrammetry (NPG). EPG was first described by Lie and Jemt in 1994 as a method for measuring implant framework misfit using a calibrated camera and high-precision analytical plotter (Lie & Jemt, 1994, no duplicate citation). Subsequent laboratory studies incorporated custom-made lightboxes, DSLR cameras, and machined abutment markings to enhance precision (Agustín-Panadero et al., 2015; Rivara et al., 2016). Advances in digital photography and software have since led to the commercialization of EPG systems, each employing different technologies and scan body markers.
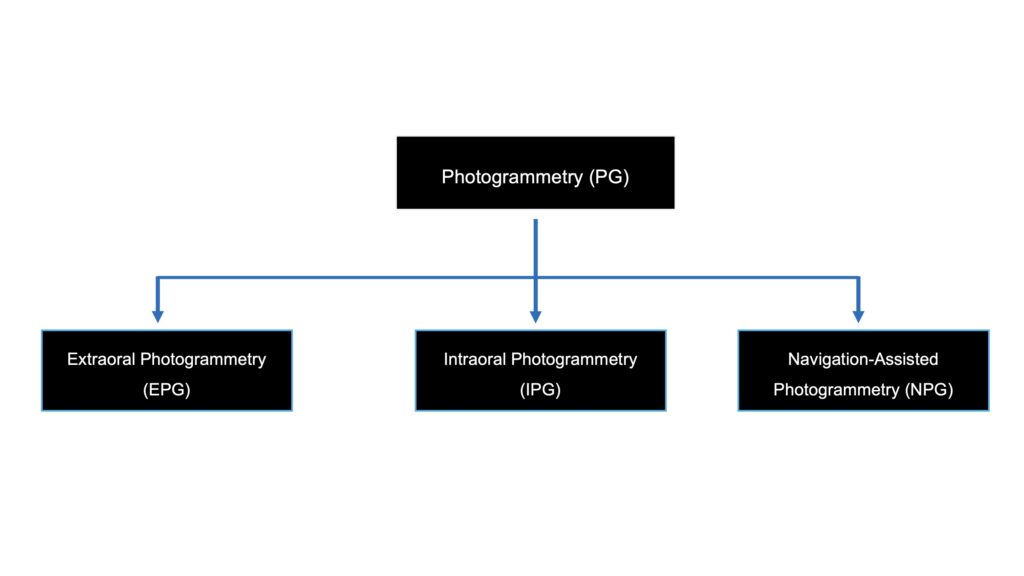
Fig. 1: Types of photogrammetry systems
Extraoral Photogrammetry (EPG)
The PIC system, launched in 2010, was the first commercial EPG device. It uses a stereo camera with two charged-coupled device (CCD) sensors specifically designed for clinical use, capable of detecting coded, flag-shaped scan bodies attached to implants (Pozzi et al., 2025a; Fu et al., 2025). Both one-phase and two-phase PG impression protocols yield comparable linear and angular deviations, making either suitable for complete-arch prostheses (Jiranaphawiboon et al., 2025).
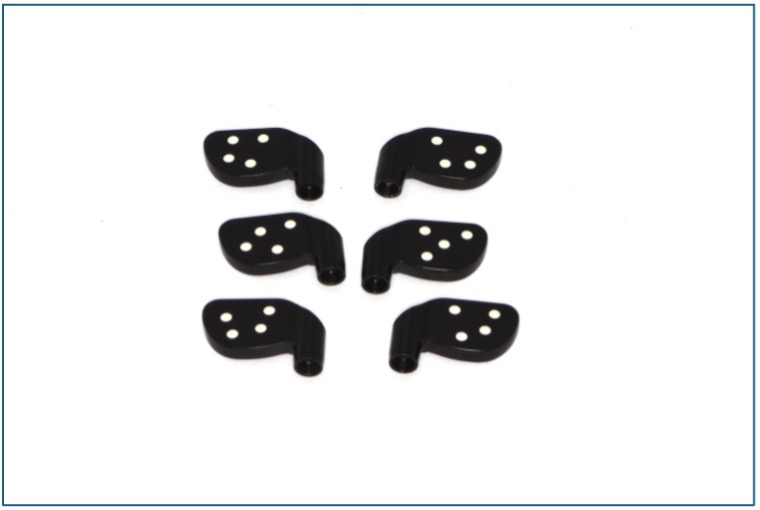
Fig.2: Extraoral photogrammetry, PIC Dental [PIC System, Spain (1st generation)]; (a) PIC high-performance thermoplastic polymer SB characterized by black flag-shaped scan bodies with white dots 
(b) PIC scan bodies on model
The iCam4D system (Imetric), introduced in 2018, combines PG with structured light scanning and calibrated radiopaque titanium SBs. Its open digital workflow and ability to accommodate mandibular flexure make it a dependable option for full-arch implant rehabilitation (Pozzi et al., 2024; Revilla-León et al., 2021; Negreiros et al., 2025). Several studies and systematic reviews have reported favorable clinical outcomes and regard EPG as a reliable method (Gómez-Polo et al., 2023; Hussein, 2023; Rutkunas et al., 2023). Numerous investigations have demonstrated superior accuracy and reliability compared with IOS (Fu et al., 2025; Negreiros et al., 2025; Zhang et al., 2023). Reported performance varies between devices: the PIC system shows trueness values of 10–49 μm and precision of 5–65 μm, while the iCam4D system demonstrates trueness of 24–77 μm and precision of 2–203 μm (Negreiros et al., 2025). Despite its precision in capturing implant positions, EPG still requires an additional IOS or conventional impression to record soft tissue contours and occlusal relationships.

Fig.3: Extraoral photogrammetry, Icam4D [Imetric, Switzerland (3rd generation)]; (a) Icam4D radiopaque titanium SBs. 
(b) EPG camera system combines structured light and photogrammetric scans to capture three-dimensional data 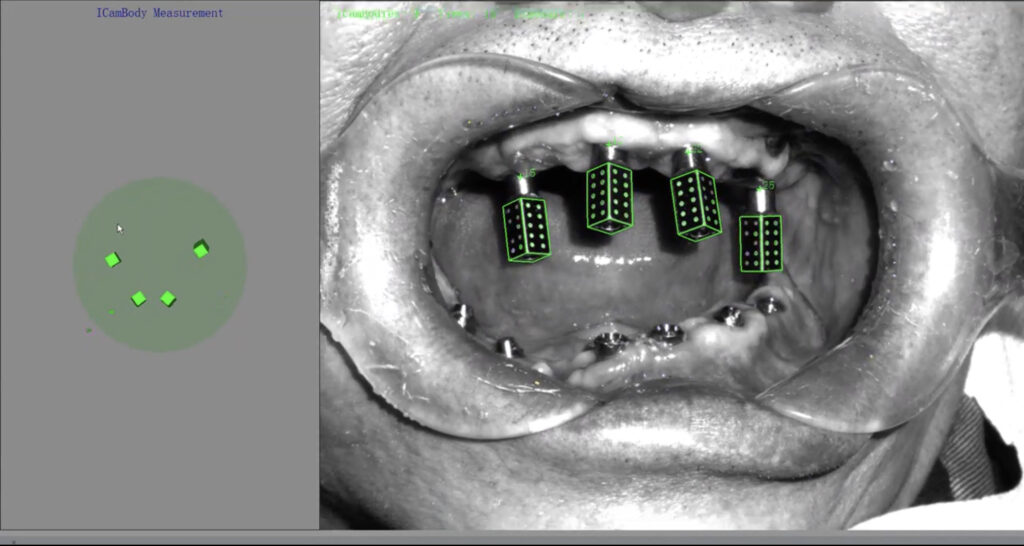
(c) The exact position of EPG scan bodies is automatically identified by the software
Intraoral Photogrammetry (IPG)
To address this limitation, recent developments have integrated PG directly into IOS devices, leading to the invention of IPG. Rather than scanning the actual geometry of the SBs, IPG systems detect coded markers on high-accuracy scan bodies (HACS) (Fu et al., 2025). Despite statistical differences, trivial linear discrepancies (31–39 µm) indicate that inter-implant SB distance might not be clinically relevant in complete-arch implant scan accuracy, including angular trueness and precision (Revilla-León et al., 2025a). Similarly, ambient lighting has been shown to influence trueness, but differences remain clinically negligible (Gómez-Polo et al., 2023 — corrected). Both in vitro (Fu et al., 2025) and in vivo (Eldabe et al., 2025) studies have demonstrated that the accuracy of IPG is comparable to EPG and significantly higher than IOS.

Fig. 4: Intraoral shining photogrammetry, Aoralscan Elite (Shining 3D, China); (a) IPG scan bodies on model. 
(b). High-accuracy coded scan body (HACS) has a hexagonal vertical shape and a multi-faceted horizontal part with black-and-white fiducial markers for accurate recognition. Automatic alignment of the HACS onscreen, converting their positions into implant coordinates according to the selected abutment type. To ensure simultaneous capture, HACS of different lengths (long, medium, short) are available for the radial pattern without touching each other.
Recently introduced systems incorporating expanded scanning fields have been described; however, to date, no published clinical or laboratory investigations have independently validated these systems or verified their practical implications for implant position capture.
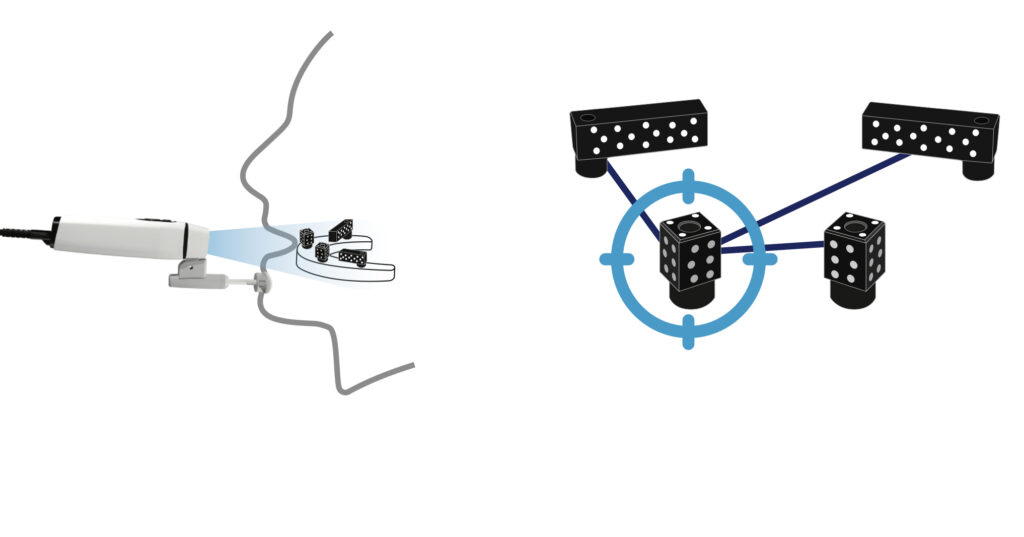
Fig. 5: Intraoral photogrammetry (38), DOF Freedom Air (DOF, Korea); Precise Implant Measurement guide tools to complete the scan outside the mouth (Left) and Intraoral scan bodies (Right)
Navigated Photogrammetry (NPG)
With the advancement of implant navigation technology and its integration into implantology, navigated photogrammetry (NPG) systems have emerged (Revilla-León et al., 2025b). These systems enable accurate capture of scan body positions and superimposition of virtual geometry onto patient anatomy through dynamic tracking and navigation. Immediate post-operative NPG scanning allows automatic integration of implant coordinates with pre-operative digital datasets in a streamlined workflow (Revilla-León et al., 2025b). Soft tissue scans remain optional but may improve laboratory accuracy, particularly in full-arch rehabilitation, as data integrates seamlessly with prosthesis design software for virtual wax-ups.
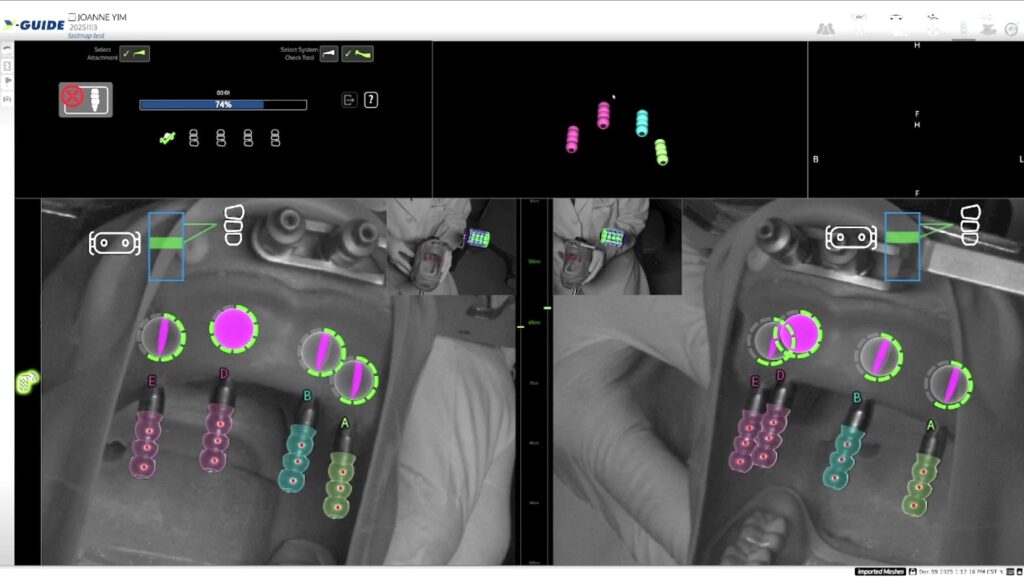
Fig. 7: Navigated photogrammetry Fastmap® (X-Nav Technologies, USA) scan bodies; (a) NPG Fastmap® scan bodies are attached to the multi-unit abutments and positioned within the overhead camera’s field of view, ensuring correct alignment of the three red markers on each scan body (scanning in progress). 
(b) Once scanning is completed, the navigation system accurately registers the orientation of all scan bodies.
Conclusion
Systematic reviews demonstrate that EPG provides clinically acceptable accuracy for full-arch implant impressions and frequently outperforms conventional and IOS approaches while improving efficiency and user satisfaction (Gómez-Polo et al., 2023; Rutkunas et al., 2023). Preliminary in vitro investigations suggest that IPG offers comparable accuracy to EPG (Fu et al., 2025), while NPG represents a promising innovation for immediate post-surgical implant mapping (Revilla-León et al., 2025b). However, clinical evidence for both IPG and NPG remains limited. Robust, well-designed clinical studies are needed to validate performance, refine clinical integration, and support adoption in routine full-arch implant rehabilitation.




